Chapter 18 – Global Health and The Changing Contours of Human Life
Coordinating Lead Authors:[1] Ama de-Graft Aikins, Dan Wikler
Lead Authors:[2] Pascale Allotey, Gustaf Arrhenius, Uli Beisel, Melinda Cooper, Nir Eyal, Dan Hausman, Wolfgang Lutz, Ole Norheim, Elizabeth Roberts, Denny Vagero
Contributing Authors:[3] Karim Jebari
Word count: 29,837
Abstract:
The contours of human life – birth, childhood, maturity, reproduction, the experiences of health, illness, and disability, and death – have been and will remain nearly universal; but their duration and texture are undergoing great changes. In this chapter, we chart the transformations and make projections into the near future. Many of the trends are favorable: fewer children are dying, and many enjoy greater longevity. But these advances are not distributed uniformly among and within countries and regions. Furthermore, the value of longevity is compromised by an increasing number of people living with diminished health under inequitable systems of health and social care. A more just future can be achieved by a continuing emphasis on equity in global health systems even as human lives continue to be extended and enhanced.
Introduction
For all of the great variations in history and culture among the world’s peoples, and despite momentous changes in society, technology, and the environment over the past several hundred years, most human lives have had similar contours. We are conceived and born; if we avoid premature mortality, we go on to live as children, then as adolescents, then as adults; we form relationships based on kinship, love, and friendship; most have children of our own; we age; and we die. Each of us can respond with recognition and emotion to the stories and literatures of peoples remote from us in geography and time.
In the decades to come, these common patterns will continue to structure human lives, but their rhythms and textures will change greatly for many, reflecting personal and social consequences of economic growth, of scientific and technological advances, and the continuing evolution of political and moral aspirations and norms. In the main, these are welcome developments. Whereas two centuries ago in the richest nations and much more recently in less affluent parts of the world, parents could expect to see many of their children die, along with, not infrequently their mothers, infant mortality rates are now below 1/100 in the vast majority of countries, and maternal death rates are in most countries well below 1/1000. People everywhere can expect to live longer and healthier lives. Raising children, which used to occupy a large part of people’s adult lives, now occupies a third or a half. Literacy is widespread, and the whole world can be in rapid contact via electronic media. Further improvement in the duration and quality of life, including the avoidance of illness and disability, are likely to be augmented by both biological and technological enhancements of our capacities. In this chapter, we chart some of these advances, and make projections into the near future.
As impressive as these gains have been, however, their distribution across and within human societies has been staggeringly uneven. Identifying these inequalities serves both to identify important trends in these key concerns of each human’s life and to contribute to a moral agenda dedicated to bringing these benefits to all.
A note on concepts and measures of inequality:
Following the approach adopted in chapter 3 on “Inequality and Social Progress”, the conception of inequality used in this chapter is objective (not merely perceived), static (not dynamic), and relative (not absolute). Note however that at different points, the present chapter uses different notions of equality and of distributive justice in health. Using either Chapter 3 or philosophical parlance (Cohen, 1989; Lippert-Rasmussen and Eyal, 2012) the differences pertain to how things are distributed (the distributive “pattern”), what is being distributed (the distributive “currency”), and to the area in which that assessment is made (the distributive “locus”).
- The distributive pattern: Sometimes we focus on the gap or inequality in health as a morally significant fact in itself. Other times we emphasize the avoidable health gaps exposed or caused by health inequality, especially in the case of those persons or populations who are worse off. The latter can reflect a straightforward utilitarian approach or a prioritarian approach. Prioritarianism puts greater weight on the health or well-being of those who are worse off rather than focusing specifically on the gap between them and those who are better off. At other points in this chapter we emphasize the avoidable or even intentional wrongful human and structural barriers to better health which inequality merely exposes. For example, inequalities in numbers of injuries may reflect officially-sanctioned violence against minorities. When we indicate inequalities in terms of various indices, that usually reflects pragmatic measurement needs rather than deeper thoughts on what fundamentally constitutes a health inequality, or the one that matters.
- The distributive currency: The chapter focuses on inequalities in the availability of health services, but we also explore inequalities in other distributive “currencies”, such as longevity or freedom from disability. Additionally, we discuss inequalities in probabilistic spaces like life expectancy and risk of disability. Our chapter lays emphasis on equality of true access to services. Cases in point would include ramps that equalize access to health facilities by wheelchair-reliant patients and language translators who equalize access across linguistic line. An alternative emphasis is on equality in the resources being offered to all, for example, in whether all are allowed to use the staircase to the clinic. Related to the question which currency is being used is the question whether many currencies matter. We sometimes focus on equality in a single component of health (e.g. in diabetes status, in ambulatory functioning), potentially suggesting that these may matter independently of one another. Other times, what we assess is equality in a summary measure of health (e.g. in overall disability status), or even in a related summary measure of utility or capability to which health is only one contributor (e.g. in welfare or in health-related quality of life). In current philosophical debates concerning equality, one also finds a very different notion of equality that focuses on equality of fundamental social status. Although distinct from a concern about distribution of fungible goods and services, fundamental equality in the relations among members of a population is rarely obtainable when inequalities in money, power, and, to some degree, health and health care, are large.
- The distributive locus: The present chapter is concerned both with inequalities within districts, countries, and regions of the world and with inequalities between them. Sometimes we discuss inequalities among individuals, as is common in economics (inter-individual inequality or, per chapter 3, “vertical inequality”), but usually we focus on inequalities among social groups (inter-group inequality or “horizontal equality”). The groups whose health or access to health care we compare include different income quintiles, levels of education, different racial and ethnic groups, and different genders. These groups are marked out either by their tendency to attract advantages and disadvantages across many distributive spheres, or by their social salience and relevance to personal identity. That said, often these two group definitions overlap (e.g. when a racial minority group is both socially salient and faces multiple disadvantages). Sometimes we focus on inequalities in contemporaneous health states but we do so largely for pragmatic or measurement reasons: what ultimately matters with respect to health (as opposed to access to health care) is inequality in lifetime health or inequalities within life stages. Sometimes we examine inequalities in the prevalence of certain health states (such as living with HIV). At other times we assess inequalities in the incidence of health states (such as when HIV infection took place).
1. Coming into being
Children and adolescents represent almost a fourth of the world’s current population (United Nations, 2015). Almost 90% of them live in low- and middle-income countries, which continue to face multiple social, economic and health challenges. Although child mortality rates have fallen worldwide since the turn of the millennium, the burden of under-5 deaths is still disproportionately concentrated in sub-Saharan Africa and South Asia (UNICEF 2014: 5). Moreover, significant disparities can be identified within these regions, where the highest birth rates and the vast majority of child deaths occur at the lowest quintiles of the wealth and income scale (You and Anthony 2012: 12; UNICEF 2014: 22). The number of adolescents – that is, young people aged between 10 and 19 - has now reached an historical all-time high and 90% of these live in developing countries. However, it is projected that the population aged 12-24 will soon decline in all major regions except Africa (United Nations 2012: 4). As a result, Africa’s share of the world’s adolescent population is expected to rise from 18% in 2012 to 28% in 2040. This concentration of the world’s young people in Africa is likely to have profound health implications because it is occurring in a region marked by extreme inequalities and high youth unemployment. This section of the report focuses on how humans ‘come into being’ in today’s world: on child mortality and health, adolescent mortality and health, and on the inequalities pertaining to these fields.
1.1 Infancy and child mortality
During the last half century, major progress has been made in the reduction of global child mortality with an overall decline of slightly more than two-thirds occurring between 1970 and 2013 (Wang et al. 2015: 961, 973). The under-five mortality rate has almost halved since 1990, dropping from 90 to 46 deaths per 1000 live births between 1990 and 2014 (UNICEF 2014: 5). In most regions, the greatest absolute declines have been reported among the poorest households, with the notable exception of sub-Saharan Africa.
Yet despite these promising trends, there remains significant cause for concern. The absolute burden of under-five deaths is still astonishingly high: worldwide, 223 million died before the age of five between 1990 and 2013 (ibid). These premature deaths are overwhelmingly concentrated in sub-Saharan Africa and South Asia, which together account for 4 out of 5 under-five deaths worldwide. 1 in 11 children in sub-Saharan Africa dies before age 5, compared to 1 in 159 in high-income countries (ibid). The vast majority of these deaths are preventable. Proven interventions exist to avert the most common causes of unnecessary death among children and adolescents – from pneumonia, diarrhoea, malaria and HIV/AIDS to road injuries and drowning – pointing to continued failures of political will and global coordination.
Moreover, the global reduction in child deaths continues to elude the youngest of children. Neonatal deaths – that is deaths occurring in the first 28 days of life - make up almost half of all under-five deaths and are declining more slowly than other childhood deaths (UNICEF 2014: 5-6). At a worldwide level, preterm and labour-related complications account for almost 60% of neonatal deaths. These complications are correlated with the education level of the mother and are more common among low-income, rural households.
Globally, large disparities in child survival exist between countries. With 157 deaths out of 1,000 births Angola is the country with the highest under-5 child mortality in the world, while Finland, Iceland, Luxemburg with 2 deaths have the lowest mortality (UNICEF, 2015: 24-25). “A child born in the highest under-five mortality country faces about 80 times the risk of dying before age 5 as her or his counterpart in the lowest mortality country” (ibid: 27). Inequalities also exist within regions and even within countries. Within the European Union, for instance, infant mortality is highest in Romania with 9.8 deaths per 1 000 live births and the lowest in Finland with 2.3 (European Union, 2013: 18). This trend also pertains to child deaths where Romanian children also experienced the poorest survival chances in the EU in 2010 with 37 deaths per 100000 population for boys and 30 for girls. Child death rates have dropped to as low as 10 among Slovenian boys and seven for Danish girls (ibid:21).
The continued high incidence of infant and child death in some countries plays a significant role in determining how personhood is bestowed over time, sometimes at a child’s first or even fifth birthday, instead of at birth (Scheper-Hughes 1993; Conklin and Morgan 1996). These practices of gradual personhood contrast sharply with the trend toward marking child, infant and even “prenatal” death much earlier in wealthier countries, through funerals, and other forms of memorialization, as infant and child death becomes comparatively rare (ibid).
The Millennium Development Goals (MDGs) were heavily focused on child survival. The fourth of these ambitious goals was to reduce child mortality (under five mortality) by two thirds between 1990 and 2015. Many countries, such as Bangladesh and China, managed to reach this goal while others, such as India, did not. The world, taken as a whole, also failed (United Nations 2015). So while we can observe that worldwide overall child mortality has been decreasing significantly since the 1970s, a closer look at this trajectory reveals a more complicated spatial picture of ongoing progress in some countries and regions punctuated by significant setbacks in others. Furthermore, progress has not been continuous in a temporal sense. The reduction in child mortality began to slow down in 1985 and reversed direction in 1994 (-1/2%) before resuming its former downward trend beginning in 1997 (ibid.).
How do we explain this interruption of more than a decade?
1.2 Child mortality and the changing contours of global public health
The 1980s and 1990s were the period in which global financial institutions such as the World Bank and IMF used debt restructuring (known as Structural Adjustment Programs or SAPS) to force through draconian “reforms” of the public health sector throughout the global south. These reforms included mass privatizations, cutbacks in public spending, public sector employee redundancies, user-fee systems of health care access and a preferred model of public-private partnership in health care provision leading to the “NGOization” of the health care sector (Pfeiffer and Chapman 2012). This regime had dramatic negative effects on public health, leading to a visible deterioration of public health indicators across Africa, the former Soviet Union and other countries in the throes of economic liberalization (Kim, Millen, Irwin and Gershman et al. 2000). The evisceration of the public health sector across the global south – combined with mass unemployment, growing inequalities, and the imposition of a new intellectual property rights regime at the hands of the World Trade Organization – could not have occurred at a less auspicious time. Many countries affected by World Bank debt restructuring in the late 1980s and 1990s were also facing a significant HIV/AIDS epidemic and found themselves without the means to implement any effective response. As a result, countries, especially in sub-Saharan Africa, saw horrific increases in child and adolescent mortality during this period (Farmer 2001; Poku 2006).
By the turn of the millennium, as the devastating impact of the World Bank’s policies became difficult to ignore, this model came under increasing scrutiny. The adoption of the Millennium Development Goals (MDGs) by the United Nations in 2000 signalled a new resolve to develop a more progressive global health strategy at odds with the brutal fiscal conservatism of the World Bank. Under the strain of overwhelming criticism, the World Bank itself adopted a new focus on the social aspects of growth, initiating what some refer to as the post-Washington consensus era in global development policies (Bedford 2009: 2-13). This turning point coincided with the arrival of a new set of institutional actors, including new private foundations such as the Gates Foundation, new national and global programs to combat specific infectious diseases, and new global alliances such as the Global Alliance for Vaccines and Immunization (GAVI), which have together profoundly transformed the landscape of global health interventions (McCoy and McGoey 2011; Williams and Rushton 2011). This new global health complex has reinvested in health care at a time when states have retreated, and has generated a renewed focus on infectious disease research among pharmaceutical companies, who had neglected the area for many years. As a consequence of their interventions, we have seen remarkable progress in the treatment of HIV/AIDS, neglected tropical disease and other infectious diseases and faster than expected decreases in child and adolescent mortality. Mortality from infectious disease among children and adolescents remains high, but appears to be steadily declining. Child deaths from HIV/AIDS peaked in 2005 and have declined thereafter, no doubt as a consequence of greater access to anti-retroviral treatments.
However, there are significant limitations in this new model of global public health. New institutional actors such as the Gates Foundation have no doubt made important contributions to the prevention and treatment of infectious disease and have had a marked positive impact on slowing the progression of HIV/AIDS in particular. At the same time, these actors have adapted to, rather than restructured, the public-private infrastructure of health care imposed by the first-generation Washington consensus, and they continue to rely on a mix of non-profit, philanthropic and private (pharmaceutical) entities to address public health issues. The new global health actors work in close collaboration with big pharma and are in an important sense driven by the desire to generate a new regime for pharmaceutical innovation and a new stream of revenue flows for the pharmaceutical industry, which has been faced with an innovation deficit and expiring patents for more than a decade now. In this way, “public health” is being resurrected as a profitable area of investment in ways that shape the kinds of health care interventions that are prioritized and foreclose the revival of a truly public health-care infrastructure. This has resulted in overwhelmingly vertical funding schemes focused on single diseases and a prioritization of distinct, commercializable medical interventions over environmental or infrastructural improvements in public health. While these schemes have contributed significantly to the decrease in child mortality overall, the vertical orientation has equally created an uneven and fragmented health care landscape, fragmentation of actors, a new dominance of public-private initiatives and other parastate actors over national actors (Geissler, 2013; Rees, 2014), and a move towards ‘projects’ as units of action (Whyte et al, 2013; Krause, 2014), resulting in an uneven geography of “the global health complex” (McGoey, Reiss and Wahlberg, 2011). To illustrate these shortcomings, we will now look at child and adolescent health and development in more detail.
1.3 Infancy health and development
As we have seen, the problem of child mortality has by no means been resolved at a global level. However, most children survive even in the poorest of countries, thus addressing survival and avoiding early death is not sufficient. The development and health of children who survive are equally important. In this respect, the new Sustainable Development Goals (SDGs) (United Nations 2016) offer a much more rounded perspective than the MDGs did, addressing issues relating to development over and above the reduction in mortality.
The epidemiologist David Barker (1938-2013) is responsible for popularizing the idea that foetal and infant development is formative for later social and health careers (Barker 1989 and 1992). Barker hypothesized that environmental influences, such as nutrition, interact in utero with genetic factors to program development, a process then referred to as “biological programming.” The theory was originally attacked by both geneticists and social epidemiologists, the latter arguing that Barker failed to account for social influences on development (Ben Shlomo and Davey Smith 1991; Susser and Levin 1999). In fact, Barker was fully aware that biological programming was a process that was socially stratified and tied to family social circumstances. However, he overstated the reach of his hypothesis (Barker 1990) and claimed, in a paper in 1991, that health inequalities are already programmed in utero (Barker 1991), a claim which has been heavily criticized since (Vågerö and Illsley 1995).
The vast amount of work that was triggered by the formulation of the foetal origin hypothesis has led to its reformulation in the form of a “developmental origins of adult disease hypothesis.” According to the so-called DOHAD hypothesis, adult disease is heavily influenced by what happens during the first part of your life. Already in 1934 this insight was formulated in an influential paper in the Lancet (Kermack, McKendrick, and McKinlay 1934) which suggested that the first fifteen years of life shape survival chances in later life. The modern DOHAD hypothesis simply recognizes the fact that that social and environmental factors influence child development in a broad way, and through this process also influence adult health, in particular circulatory disease and diabetes (Barker 2013). The biology of the process is better understood today with the rise of epigenetics, which explores the ways in which that the environment “talks to” the genome and influences gene expression (Carey 2011). Nutritional shock, trauma and infections are examples of external factors that may trigger epigenetic change in children and affect their long term development. A controversial issue is whether or not such epigenetic change can trigger a response in later generations (Pembrey, Saffer, Bygren 2014; Davey Smith 2012).
If epigenetic processes can indeed exert such broad influence, programmes targeting children and overall economic development may have long-term consequences for adult health and survival. A focus on school is certainly necessary, but at the age when children normally start school the earliest environmental influences on children have already been at work for several years. Attachment between child and parents (Roisman and Fraley 2012), children’s language skills (Laplante, Barr and Brunet 2004), and non-cognitive social skills (Heckman, Stixrud and Urzua 2006) are all influenced by parents’ experience. At the same time, those factors are also determinants of children’s development, including their long term health.
War, famines and trauma represent large scale social influences that have the potential to influence public health broadly. The death toll of a famine can be appalling, but famine is likely to have a long-term influence too. Children who survived the famine during the siege of Leningrad, 1941-44, suffered “Leningrad siege hypertension” decades later. As adults their mortality from circulatory disease was elevated (Vågerö, Koupil, Parfenova and Sparén 2013). Children who survived the Ukrainian famine of 1932-33 were more likely to suffer diabetes as adults than children who were not exposed to the famine (Lumey, Khalangot and Vaiserman 2015). The “great leap forward” in China led to mass starvation in 1959-61; children born during those years were more likely than other children to develop schizophrenia as adults (Xu, Sun and Liu 2009). The modern world has failed to leave war and famines behind. Their consequences are likely to stretch long into the future. Children who survive such catastrophes and manage to live a normal life later may nevertheless be scarred by their experience in a way that impairs their health and wellbeing decades later.
1.4 Child health
Much of the recent success in reducing child mortality can be attributed to the rapid scale up of interventions designed to prevent mother-to-child transmission of HIV. In the US and other high-income countries, mother-to-child transmission has been virtually eliminated thanks to the development of an effective prevention regime (Mofenson and Cotton 2013: 1). The extension of this prevention regime to resource-poor settings has been a major focus of global health since the turn of the millennium and has achieved extraordinary success. As a result of targeted investments, new childhood infections have declined by 40% each year since 2003 (Chi, Stringer and Moodley 2013; Wang et al. 2015: 969). In sub-Saharan Africa, where there is the greatest proportion of childbirths to HIV-infected women, HIV infections by mother-to-child transmission dropped from 38% in 2000 to 15% in 2014 (UNICEF, 2015). Despite these tremendous gains, the absolute numbers of children infected with HIV remain appallingly high with 222,000 newly infected children each year, the overwhelming majority (88%) of whom live in sub-Saharan Africa (ibid.).
Global health inequalities in child health remain pertinent, children from sub-Saharan Africa, South Asia, lower-income countries and fragile contexts still have the highest under-five mortality rates (UNICEF, 2015), as well as being disproportionally affected by disease, ill-health and unhealthy living environments. However, health inequalities within countries are wide-spread too, nuancing global country league tables beyond national and regional comparisons.
Ghana is an instructive example. While economic growth has averaged 7% over the last decade, with the result that Ghana is now labelled as a low-middle income country, economic disparities are not only persistent but in some areas widening (UNICEF, 2014; Aryeetey and Kanbur, In Press). Poverty reduction has mainly succeeded in the country’s more urbanised South, while in the agricultural North little progress has been reported. Yet the majority of the population continues to live in rural areas and depends on agriculture. In fact, poverty has actually increased substantially in the Upper West region, the poorest in Ghana, provoking the World Bank to declare that Ghana‘s success story in reducing poverty is confined to its southern and urban areas only (World Bank 2011, quoted in UNICEF, 2014: 2).
In addition, Ghana’s “2010 Population Census found that just over 86% of Ghana’s workforce are employed in the informal sector, making both job security and revenue generation a substantial challenge” (UNICEF, 2014: 3). The economic gap between urban and rural, and formal and informal sector is starkly visible in health trends and outcomes in the country. A recent comprehensive survey of living conditions and health in the capital of Ghana, Accra “using pooled birth history data from Demographic and Health Surveys and the Women’s Health Study of Accra” calculated that in Accra under-five mortality “ranges from 21 per 1,000 in some parts of the city to 78 per 1,000 in other areas within the city” (Weeks et al., 2013: 6).
Such large disparities in health services and outcomes are not confined to economically poor countries, but can be found in countries throughout the world. In the United States of America, for instance, access to health services for children is highly unequal. While only six percent of white children are uninsured, 19% of Latino, 13% of American Indian/Alaska Natives, and nine percent of African-American children do not have health insurance (Flores and Lin, 2013). Overall, minority children were significantly less likely to receive specialty care than white children (ibid: 7). In addition these inequalities are compounded by socioeconomic disparities, where “Blacks and Hispanics have far higher rates of poverty, near-poverty, and low educational attainment than do Whites, for example, and are underrepresented at higher levels of income and education. Given these differences in income distributions, the shorter average life expectancy at age 25 for poor adults applies to more than 1 in 5 Black and Hispanic adults and fewer than 1 in 10 White adults” (Bravemann et al., 2010: S192). In the European Union stark inequalities can also be observed. These disparities exist both between regions and countries, as well as within countries, unfolding alongside social and economic disparities. For instance, while the average life expectancy for men in the EU was 77.0 years and for females 82.9 years (European Union, 2013: 10), this varies hugely between countries. Male life expectancy at birth varies by 11.8 years across the EU. It is lowest in Lithuania, where men live 9 years under EU average, and highest in Italy with 2.9 years over the average. For women the gap was smaller with only 7.9 years divergence. “Female life expectancy was lowest in Bulgaria — 5.5 years below that for the EU — and 7.9 years or 10 % higher than in Bulgaria in both France and Spain — i.e. 2.4 years above the EU average” (ibid.).
These inequalities within regions and countries in child mortality and health draw our attention to the fine-grained geographies of health care access and quality, as well as to how health prospects intersect with race, gender and economic status. Furthermore, they point to the importance of going beyond country and region wide league tables in evaluating progress in child mortality and health.
1.5 Adolescent mortality and health
The health experiences and needs of adolescents are sometimes continuous with those of children, but they are sometimes dramatically distinct. Infectious diseases remain among the leading causes of death in this age group. Lower respiratory infections rank among the top five causes of adolescent deaths in all regions except for high-income countries and the Western Pacific Region, with more deaths occurring among younger adolescents (under 14). Diarrhoeal diseases are also a significant cause of mortality, particularly in 10-14 year olds. In this age group, diarrhoeal diseases, lower respiratory infections and meningitis together account for about 20% of deaths in in the African and South-East Asia regions (WHO 2014: 7-9; Kyu et al. 2016: 282).
In other respects, however, mortality rates amongst adolescents evidence distinct singularities. One area of particular concern is the rise in HIV/AIDS mortality among adolescents, which has increased since 2000, bucking the overall trend towards improvement visible among all other age groups (Kyu et al. 2016: 283). Most of these premature deaths are concentrated in the African region. Further empirical research is needed to determine what factors contribute to this trend. It is possible that the increase in adolescent deaths reflects improvements in the treatment of paediatric HIV, as infected children survive into the second decade of life. It may also reflect the relative paucity of sustained treatment programs for adolescents who have survived childhood with HIV (WHO 2014: 3). Adolescents who were infected in childhood face particular challenges in adapting to the realities of chronic disease and in accessing successive antiretroviral drug regimens, particularly given the existence of extensive drug resistance in multi-drug-treated children. Adolescent HIV care must focus on morbidity related to long-term HIV care and treatment adherence (Mofenson and Cotton 2013).
Having noted these differences, it is important to recognize that mortality rates among adolescents are much lower than those of children and have shown a slight decline since the turn of the millennium. Instead, what matters most for public health interventions targeted at adolescents is the distinct set of vulnerabilities and the disproportionate burden of illness that emerges at this age. When we look at the most recent data on the global burden of disease, collected for 2013, we find that more than 80% of overall deaths among those under nineteen were accounted for by younger children, while adolescents represented more than 60% of years lived with disability (Kyu et al. 2016: 268). The leading causes of disability-adjusted life years lost among this age group are depression, road injuries, iron deficiency anaemia, HIV and suicide (WHO 2014). A recently concluded systematic analysis of the Global Burden of Disease 2013 study focusing on adolescent health, showed that alcohol misuse was the highest risk factor for DALYs for young people aged 20–24 years, while unsafe sex as a risk factor increased from the 13th rank to the second for both sexes aged 15–19 years from 1990 to 2013 (Mokdad et al, 2016: 2383).
During these years, gender, sexual practice and sex/gender identity begin to play an important role in shaping experiences of health and exposure to health risk. For instance, during adolescence there are significant health differences between girls and boys. This is a time in which young people make significant steps towards independence. Many young people have their first sexual experiences in adolescence, while many young girls get married or give birth during these years. With particular force after the age of 14, gender differences and gender/sexual identification begin to play a salient role in shaping health experiences.
At this age, we begin to see significant gender differences in rates of injury and death from interpersonal violence, with adolescent girls experiencing much higher rates of emotional and physical violence from intimate partners, while adolescent boys encounter increased risk from physical violence by other boys or men. The continued presence of female genital mutilation (FGM) is one example of gender-based violence that is still present in an estimated 28 countries, mostly on the African continent and Yemen (Muthumbi et al, 2015). While the African Charter on Human and People’s Rights on the Rights of Women in Africa recognises FGM as a violation of women’s rights and a form of gender-based discrimination (ibid: 33), an estimated 125 million women and girls have undergone the practice and many more are at risk (UNICEF, 2013).
We also see an increased vulnerability to new HIV infections between the ages of 10 and 19 and the emergence of a marked gender differentiation. Before adolescence, little difference is discernible between males and females, while after adolescence girls begin to contract new infections at a much greater rate. This trend is the same across countries but is starkest in sub-Saharan Africa, where 85% of all adolescents living with HIV were located as of 2012 (Idele et al. 2014: S145). In countries with generalized epidemics, HIV prevalence among adolescent girls tends to be much higher than among adolescent boys. In some countries in sub-Saharan Africa, more than 80% of new infections among adolescents were accounted for by girls (Idele et al. 2014: S145-S146). The overwhelming majority of these new infections are transmitted through sex. Recent research in countries with generalized epidemics indicate that adolescent girls in particular have very poor knowledge about HIV and very limited access to proven means of prevention such as condoms (Idele et al. 2014: S148-S149).
It is clear from the preceding discussion that adolescent health presents unique challenges that would best be met by targeted, gender-sensitive interventions. Yet the available data on adolescent health are extremely patchy when compared with data on children and adults, making it difficult to assess past successes or plan future interventions (Idele et al. 2014: S144-S145). Indeed, while some of the most celebrated global health interventions of the past few decades have targeted infants and in particular under-five year olds, the specific health risks of adolescents are relatively neglected both in the empirical data and in public health campaigns. This is particularly evident with respect to HIV/AIDS campaigns, where prevention of mother-to-child transmission programs have had a dramatic impact on child health and mortality, while few corresponding efforts have been made to cater to the specific prevention and treatment needs of adolescents (Wang et al. 2015: 969; Mofenson and Cotton 2013). This relative neglect has had palpable effects on the health outcomes of adolescents, where we see a marked increase in HIV infection, illness and mortality rates - especially among girls. Thus, despite the relatively low level of mortality rates in this age group, adolescents are confronted with a unique set of vulnerabilities which until recently have been somewhat neglected by the leading global health actors. For example, adolescence is the time when many people experience significant mental health problems for the first time. A recent Lancet investigation into adolescent health and wellbeing concluded that increased attention to adolescent health is crucial for the world’s future, as adolescence is “characterised by dynamic brain development in which the interaction with the social environment shapes the capabilities an individual takes forward into adult life”, thus critical for achieving human potential (Paton et al, 2016: 2423).
1.6 Conclusion
In most parts of the world, death rates among infants and young children have sharply decreased over the past four decades. Still, an infant’s chances of surviving to adulthood are strongly linked to country of birth, and death rates in sub-Saharan Africa remain very high.
Adolescents, whose numbers are at an all-time high, are vulnerable to infectious diseases affecting other children, but also experience harm from injury, violence, alcohol and drug abuse, and HIV/AIDS. The distinctive health needs of this age group is age group, including those specific to gender, remain relatively less studied and less frequently targeted compared to other children.
This progress in reducing child mortality substantially achieves the objectives of a coordinated effort, targeted by the UN’s Millennium Development Goals, and mobilized by both public agencies and philanthropists relying in large part on successful deployment of immunization and other technologies within single-disease interventions.
However, the persistence of unmet need and avoidable suffering among millions of children, concentrated particularly in sub-Saharan Africa, illustrates also some of the limitations of this approach. Achieving a world in which each newborn, regardless of place and circumstances of birth, can be expected to proceed to a healthy and vigorous childhood and adolescence will require a sustained and well-funded engagement with the weaknesses of health systems in the low-income countries and with the underlying economic, structural, and social determinants of child and adolescent health throughout the world.
2. Longevity, life expectancy and inequalities in the risk of dying
Introduction: social progress in health and longevity
People all over the world now have a reasonable expectation of living longer and more healthy lives compared to half a century ago (Peto et al. 2014). Avoiding premature mortality is possible for a majority of the world population, even for the bottom billion , given the right circumstances (CSDH 2008, , Norheim, Jha et al. 2015, UNDP 2012). This section looks at the vast improvements in global health measured as rising life expectancy, but also at inequalities in life expectancy and longevity, conceived either as differences between individuals or between groups, within countries as well as globally.
Our summary may be surprising: globally, on average, we live longer and better lives, and even if many countries and groups lag behind and some may even reverse their previous progress, overall inequalities in average-age-at death between individuals are decreasing. This reflects a two centuries old process of reduction of infant, child and early mortality, which probably represents the single most important achievement of modern man (Smits and Monden 2009). This is a reason to celebrate.
Yet, in contrast to child mortality trends, adult mortality trends 1950-2015 appear not to be converging globally; it is a much more complex and mixed picture; there is both convergence and divergence, sometimes whole regions of the world face long term stagnation or deterioration, such as in the former Soviet union, 1970-2005, or in Sub-Saharan Africa in the 1990:ies.
Within country mortality differences by income, wealth, class and level of education persist. In many countries inequalities in adult mortality increase; most typically when adult mortality improves faster among the better off. A worse scenario is when segments of the adult population in a country experience rising mortality; as has been the case in both USA and Russia recently. Much more can be done to accelerate social progress in health.
| Box 18.1: Data and methods To estimate inequality in life expectancy and longevity (age at death), we used UN Population Division (UNPD) historical life tables in its latest revision (Preston et al. 2001, United Nations Population Division 2012)[4] Inequality within each population is estimated by Le Grand’s method: Gini applied to age at death (Le Grand 1987, Smits and Monden 2009, Norheim 2010). We shall hereafter use the term longevity for age at death, and we are interested in whether inequality in longevity is increasing or decreasing.[5] Ginih can be calculated in different ways and takes the values 0 for perfect equality and 1 for complete inequality (Asada, 2007).[6] We only present results for both sexes combined. Gender inequality in mortality is an interesting field of inquiry in itself, but for ease of presentation, we do not present separate figures for females and males.[7] |
2.1 Trends in life expectancy at birth in 25 large countries (1955-2015)
Figure 18.1 shows trends in life expectancy from 1955 to 2015 for the world (thick line) and for the 25 largest countries in the world. The average improvements for the world are immense: from 48 years in 1955 to above 71 years in 2015. This is an increase of 23 years over a time span of 60 years, or put differently: more than 4 months of increase per year.
Figure 18.1 Life expectancy at birth, largest 25 countries, both sexes, 1955-2015 (Source: UNPD 2015 revision)
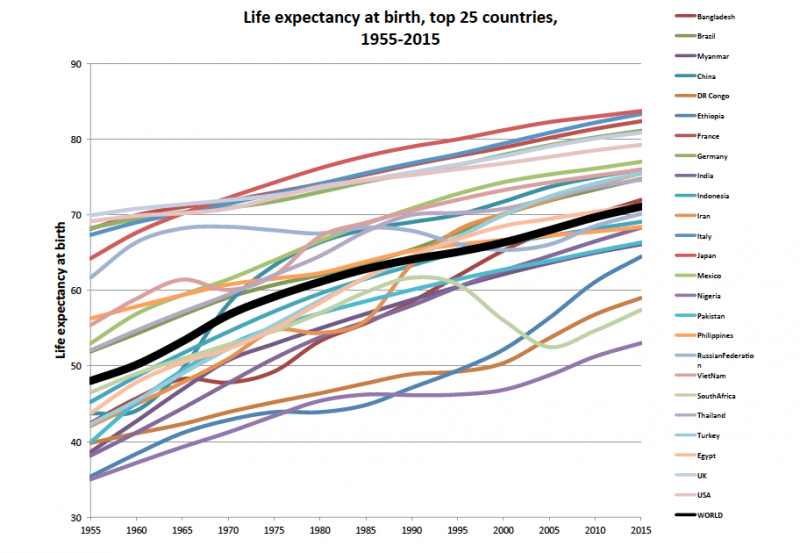
2.2 Inequality in life expectancy between countries
From Figure 18.1 we see that life expectancy differs between countries, and it looks like the dispersion is about the same in 1955 as in 2015 (about 35 years between the two countries with highest and lowest life expectancy). However, if we make pairwise comparisons in life expectancy between all 25 countries and sum up the average relative difference, as the Gini measure does, we find that there has been some decrease in inequality between countries (Figure 18.2).
Figure 18.2 Inequality in life expectancy at birth, between top 25 countries, both sexes, 1955-2015
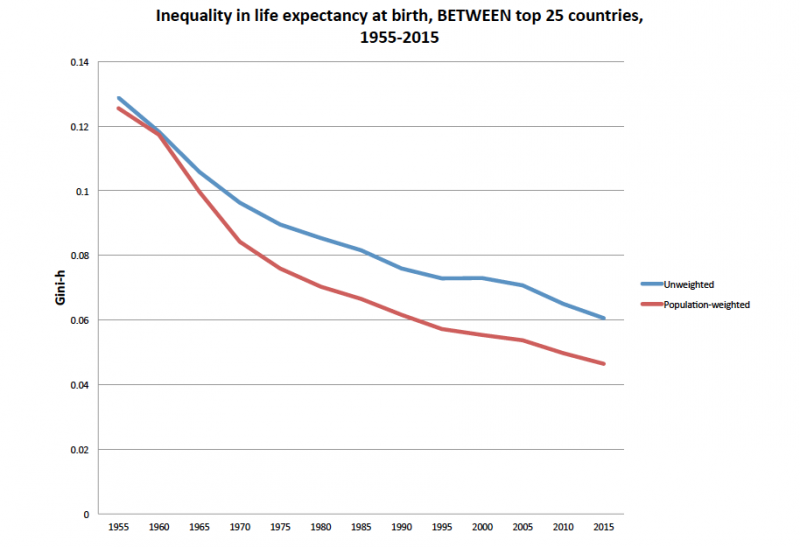
Figure 18.2 shows that in 1955, Ginih for inequality in life expectancy between countries was about 0.13 and fell to about 0.08 in 2015 (a lower Ginih coefficient represents more equality than a higher coefficient). The lower line in Figure 18.2 shows inequality between countries when they are weighted by population size. We then find even more inequality reduction by 2015 since large countries like China and India have had substantial mortality reductions at early ages and contribute more than small countries.[8]
2.3 Trends in global life expectancy inequalities
Moser et al (2005) published a comparison of life expectancy trends for 1950-2000 in 187 countries, that is every country in the world with more than one million inhabitants. By population-weighted pairwise comparison of every country with every other country they could calculate a global “dispersion measure of mortality”. They did this also for infant mortality. They found that infant mortality in the world is converging, but life expectancy trends are diverging after 1990; the divergence was driven by adult mortality trends. Goesling and Firebaugh (2004) comparing 169 countries also found that mortality convergence was replaced by mortality divergence in 1990. In a recent paper by Timonin et al (2016) the conclusion was that in 36 developed countries mortality trends are strongly patterned by global region. They could demonstrate a widening east-west gap in mortality and life expectancy during the whole period 1970-2005; after 2005 it appears to narrow. This gap coincided with the East-West geopolitical division.
2.4 Inequality in longevity within World Bank income groups and world
In the income literature, there is an important distinction between inequality within populations and between populations (Tarlo, 2003). Within- and between-group inequality is also important for health. If we compare life expectancy (= average values) between countries (as in Figure 18.2), we ignore within-country inequality. This may lead to underestimation of total inequality (Figure 18.3).
Figure 18.3 Inequality in longevity, both sexes, within World Bank income groups and World, 1955-2015
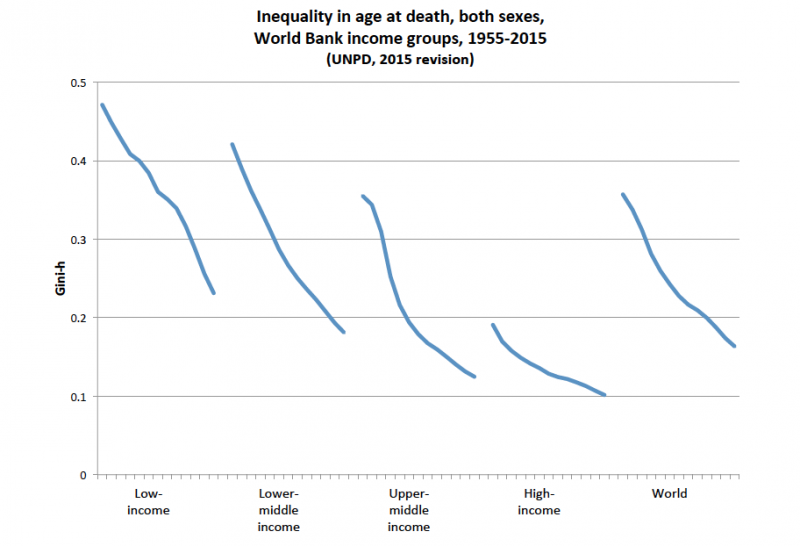
Figure 18.3 shows within inequality in longevity for the world and for each of the four World Bank income regions (low-income, lower-middle income, upper-middle income, and high-income groups). Here, we treat each group of countries (or the whole world) as one population and compare longevity for each individual within that population. We see that inequality is high, but the trends are towards more equality.
Within-group inequality for the world was much higher in 1955 (Figure 18.3, Ginih = 0.36) compared to between-country inequality (Figure 18.2, Ginih = 0.14), although both within-group and between-group inequalities fell in the period (to 0.16 and 0.07 respectively in 2015). In our view, within-group inequalities are most relevant for monitoring trends since they capture inter-individual differences, not only differences between averages.
2.5 Inequality in longevity within countries
Figures 18.4a-c show inequality in age-at-death within some of the 25 largest countries in the world. Although the trend is towards more equality, some countries are still at high levels, and there are interesting inter-country variations in patterns.
Figure 18.4a Inequality in longevity for four Sub-Saharan African countries
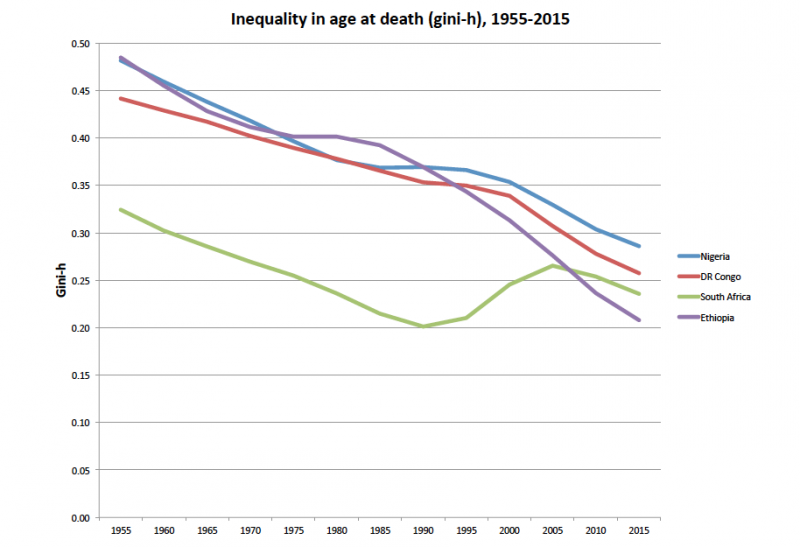
Figure 18.4a shows inequality trends in four Sub-Saharan African countries. Ethiopia’s reduction of inequality has been more rapid the last 25-30 years compared to Nigeria and the Democratic Republic of the Congo. South Africa stands out with a period from early 1990 to early 2000 where inequality increased due to very high age-specific mortality in children and young adults due to HIV/AIDS.
Figure 18.4b Inequality in longevity for four large countries

Figure 18.4b shows time trends four other large countries: India, Russia, Iran and China. Inequality in India is highest, but steadily falling. Iran’s reduction in inequality was interrupted by high adult male mortality between 1975 and 1985. China made a big improvement after around 1965, while Russia had no, or even periodically negative developments, in most of this period.
Figure 18.4c Inequality in longevity for five high-income countries
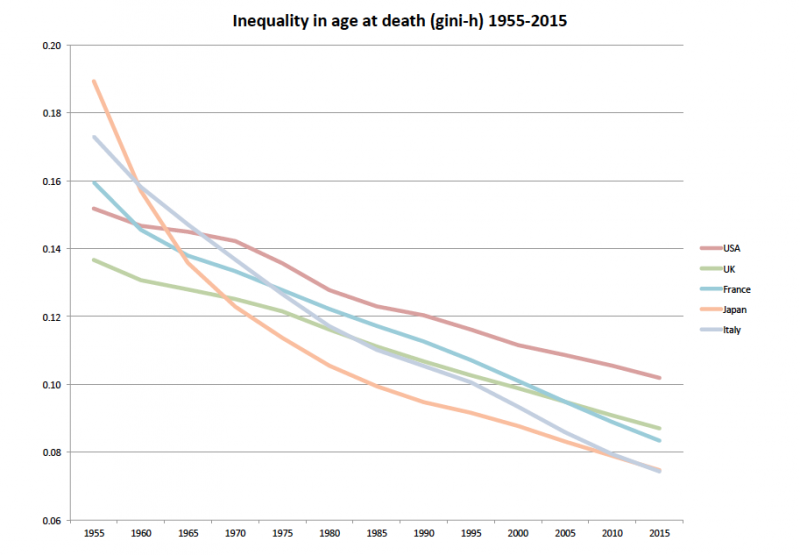
Figure 18.4c shows trends for five high-income countries: USA, UK, France, Japan and Italy. All countries are at relative low levels of inequality. Japan had high rates of decline early in the period while the US lagged somewhat behind after 1970 and up until today.
Summing up, we find that inter-individual inequality in longevity (age-at-death) within countries are decreasing. Reduction of infant and child mortality is most important for this development. Some countries still experience high inequality and some countries even had periods with rising inequality in age at death (South Africa and Russia).
Overall, we find that there is, at the same time, overall convergence in age-at-death within and between countries and increasing differences in life expectancy, driven by adult mortality trends: the survival curve for the world is mostly moving in the direction of rectangularization; but not everywhere and not in every social group.
2.6 Global inequalities in age-specific mortality
We will now look at age-specific mortality rates; the picture becomes more complex.
Figure 18.5. Relative difference in age-specific mortality rates, World, both sexes, 1990 and 2015
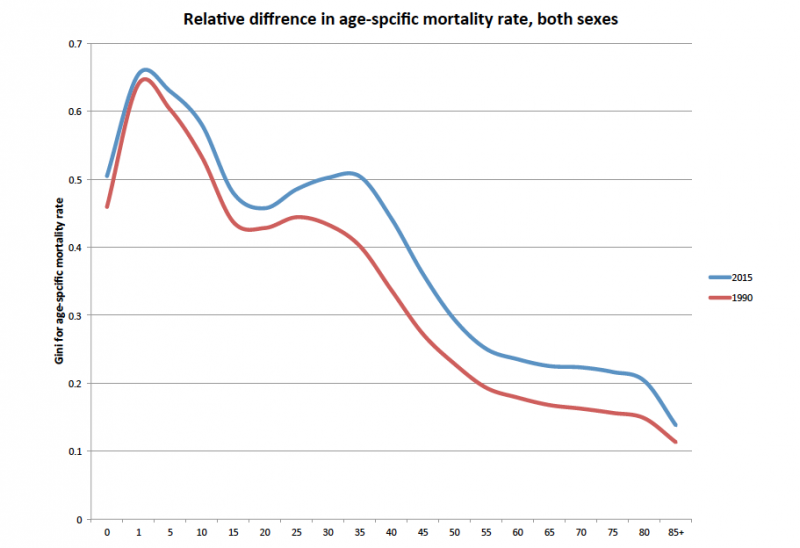
Figure 18.5 shows that the relative difference (measured as Gini) in all age-specific mortality rates between all countries in the world increased in the period 1990 to 2015. This happens when the relative decrease in age-specific mortality for countries with lower mortality is faster than for countries with higher mortality, or when there is a rise in age-specific mortality in countries with high mortality (such as in Russia 1970-2005) and a fall among most other countries. This finding is the basis for the most common description of health inequality trends within countries: health inequalities are increasing (see also next section below).[9] If inequalities in age-specific mortality increase in all age groups, inequality in life expectancy will increase.
Rising relative inequality is important for two reasons. First, even if inequality in age-at death is decreasing, the increase in relative difference in age-specific mortality rates shows that the speed of mortality improvement for high-mortality countries is slower than for lower-mortality countries. So the picture is not all positive; in particular, as can be seen from the graph, adult (ages 30+) mortality rates are more unequal in 2015 than in 1990. Second, if what we really care about is how people fare over their lifetime we must address adult and old age mortality differences among women and men and not only child and maternal mortality, as was done in the MDG:s [10] The next section looks at social group inequalities and not only overall health inequalities between individuals (as discussed above).
2.7 Inequality in life expectancy and mortality by socioeconomic status within countries
The longest series of data about social class differences in mortality is probably the decennial supplements of occupational mortality, published by Office of Population Statistics (OPCS) in Britain. The statistical series goes back to 1911 and has been published every decade up to now. The all-cause mortality of social classes I, II, III, IV and V are compared. Classes are defined from occupations. The same mortality pattern has been observed every decade: a mortality gradient is seen, in which mortality in social class V (unskilled workers) is typically about twice as high as in class I (professionals) with classes II, III and IV falling in between. The continuity in this pattern, decade after decade, in spite of a gradually changing disease panorama, impressive economic growth, modern medicine and welfare state provisions, is quite remarkable (OPCS 1995). It suggests that health differentiation is a fundamental social process, closely tied to the general stratification in society.
The “Black Report”, presented by Sir Douglas Black to the British government in 1979, and immediately dismissed by the then conservative government, was challenged to understand these regularities and to suggest means of changing the situation. Why do social class differences in health reappear again and again in every new generation? The report triggered academic and political controversy. The focus of the report was on the contribution to health of poverty and material circumstances in adult life. Some of the critique of the report argued that issues of selection were not dealt with properly. Health and vitality in early life may to some extent determine social career and contribute to the social differentiation of health in adult life. Arguments about “selection” versus “causation” were once quite bitter. The introduction of a life course perspective has changed this. Today, this conflict has been solved theoretically, by the insight that health in early life is heavily influenced by the social circumstances of the previous generation (Vågerö and lllsley 1995, Kuh and Ben Shlomo 2004). Among public health scientists today there is thus a broad consensus that life-long social circumstances have a dominant influence on people’s health and survival. It is also generally agreed that health conditions may influence economic activity and social mobility and thus reinforce the pattern of social inequalities in health (Greenhalgh, 2008).
The publication and controversy around the Black report inspired a new generation of researchers, which has resulted in a vast literature on health inequalities. It is fair to say today that social inequalities have been found in every country that has data to make a study possible. It is a general phenomenon, observable in rich and poor countries alike, on every continent and in every social system (CSDH 2008).
Social inequalities have typically been conceived as differences by occupational class, by education, sometimes by income or by area, comparing deprived and affluent areas. In very general terms the pattern is similar across different ways of stratifying the population and across different health problems, but anomalies exist and looking at specific causes-of-death, or specific health conditions, the pattern could vary considerably. Breast cancer among women, for instance, is generally higher among high-educated women than among those with low education.
Further, even if occupation, education and income are closely correlated in most societies, they cannot be interchanged for each other, which has been a common practice in social epidemiology. Education, occupation and income tap into different etiologies and predict mortality and longevity independently of each other (Geyer et al 2006). Theoretical understanding of social inequalities in health, mortality and longevity in the adult population has to allow for several determinants and risk factors, distributed across the life span and within the previous generation. There is a complex and dynamic set of relations between those factors.
Access to health data is poorest in low and middle income countries. However, the program for Demographic and Health Surveys, running since 1984, has been quite successful in providing us with child mortality by household economic level. Tanja Houweling used World Bank country reports and DHS data for 43 low and middle income countries, to compare the richest fifth of households with the poorest fifth in each country. (Houweling 2007) She found a systematic difference by family income, in that child mortality in poor household was around double that of rich households in the same country. Wagstaff et al, using Living Standard Measurement Study data for nine countries, found very similar results (Wagstaff et al, 2000). Hosseinpoor et al (2005) used regionally representative DHS data for Iran, in the year 2000, to study infant mortality by household income groups. The results showed a gradient in infant mortality from quintile 1 to quintile 5, which revealed that infant mortality is more than twice as high among the poor compared to the rich. This is the typical pattern in any country, although the estimated size of mortality differentials is sensitive to the method of defining household income (income , assets, expenditure) (Houweeling , Kunst and Mackenbach, 2003) and varies between countries.
There is scarcity of data allowing us to assess how social inequalities in child mortality change over time within many countries (Victora et al, 2003). The study by Moser, Shkolnikov and Leon (2005), using country data to estimate global trends in infant mortality, suggests that there may be a convergence in infant mortality worldwide. This is in contrast to global trends in adult mortality, which they suggest to be diverging after 1985/1990.
Trends in social inequalities in mortality/longevity within developed countries and among adults are better studied and known. It appears that the dominant trend is one of increasing mortality differences. We can distinguish four main patterns of how 1) mortality in in general and 2) social inequalities in mortality have changed during the last few decades. The first three patterns describe growing mortality inequalities. We list them by the degree of moral concern they raise, with the most problematic pattern first.
- Sharply fluctuating (falling, rising, falling) life expectancy trends nationally. Growing social inequalities in mortality/life expectancy, combined with falling life expectancy in large segments of the population.
- Increasing life expectancy trends nationally. Growing social inequalities in mortality and/or life expectancy, combined with falling life expectancy in large segments of the population.
- Increasing life expectancy trends nationally. Growing social inequalities in mortality/life expectancy, combined with increasing life expectancy in all segments of the population.
- Increasing life expectancy trends nationally, combined with narrowing of the social gradient in mortality.
The first pattern can be illustrated by Russian mortality trends 1970-2005. A long term trend of falling or sharply fluctuating life expectancy dominates from 1965 to 2005. It is combined with increasing mortality differentials by education, at least for the period 1980-2001, during which period low educated men and women experienced falling life expectancy (Murphy et al 2006). Similarly, Estonia demonstrate dramatically growing mortality inequalities both by education and by ethnicity during the 1990-2000 period, driven by rising mortality and falling life expectancy among the low-educated and in the Russian minority (Leinsalu et al 2003, 2004). South Africa probably fits this pattern too.
The second pattern can be illustrated by United States. Anne Case and Angus Deaton noted, recently, that middle aged white Americans have experienced increasing mortality during the 1999-2013 period (Case and Deaton 2015). However, this trend only applied to low educated whites, not to those of middle or high education. Behind the epiphenomenon that they observed was a longer trend of generally widening mortality differences between educational groups, and not only in middle aged men and women, since at least 1990. The mortality of white men and women with less than twelve years schooling have been growing gradually worse over time (Olshensky et al 2012).
The third pattern is much more common than the two above. Countries that are doing quite well in general life expectancy trends often demonstrate increasing social inequality in mortality/life expectancy, such as many countries in western Europe. Anna Steingrímsdóttir and colleagues (2012) published annual life expectancy data for men and women in three educational groups in Norway from 1960- 2009. This is probably the longest series of mortality differentials by education that we have. There is, broadly, a continuously growing gap between all three educational groups over the fifty year period; also the low educated group is making progress, but at a slower pace than the other two groups. Shkolnikov et al (2012) demonstrated the same pattern in a comparison of Finland, Norway and Sweden for the 1970-2000 period. In all three countries mortality is falling in all educational groups, but faster the higher your education is, resulting in a growing life expectancy gap. Leinsalu et al (2009) demonstrated the same pattern for Poland and Hungary, for 1990-2000.
The choice of inequality measures makes a difference. The study of 6 western European countries by Mackenbach et al (2003) showed a widening mortality gap by education in all of them, when using a relative inequality measure; using an absolute measure, the differences in mortality were more stable, except for Finland. Reducing absolute mortality differences should be easier than reducing relative ones when mortality rates are falling.
The long term increase in absolute mortality differences and in life expectancy between men and women of different educational backgrounds in Finland, Norway and Sweden is therefore quite remarkable. Understanding this “welfare state paradox” has become a hot research topic in social epidemiology. Perhaps global market forces and corporate actors now exercise an influence over national income distributions, labour markets, consumption patterns, taxes and welfare policies in general that is too powerful for national governments to balance?
The fourth pattern of mortality differentials and trends, outlined above, corresponds to what most governments aim for. The policy documents of WHO and of national governments will state that a major public policy goal is improved health in combination with smaller health inequalities. It appears that most governments in reality will have to cope with the first three scenarios. Moving to the fourth pattern, of growing life expectancy and smaller health inequalities is not consistent with “business as usual”, according to the influential report of the Commission on Social Determinants of Health (2008). Although policy making in this field is now intense, the way forward is not very clear.
2.8 Differential Mortality by Level of Education
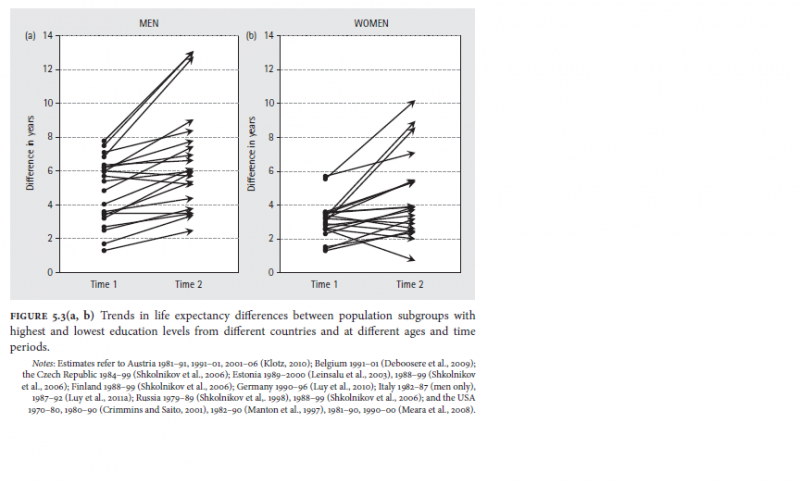
Education – one of the most important sources of observable social heterogeneity in all countries – is perhaps also the most common social stratification variable in health studies. Education leads to strong differentials in health and mortality. There is ample evidence (Baker et al 2011; Lutz and Skirbekk 2014) that education empowers people in various dimensions and thus has a direct and causal effect on health related behavior, health, mortality and longevity. In all countries of the world child mortality is significantly lower for children of more educated women even after adjusting for the effect of income/wealth (Pamuk et al 2011, PDR) and university educated men and women compared to those with basic education differ in life expectancy of up to 12 years. Figure 18.4 shows that this is the case in industrialized countries and that in most countries the differentials have actually increased in recent years.
The discussion about the welfare state paradox has highlighted the role of the modern welfare state. A number of European studies has compared the size of health inequalities in European countries. The hypothesis was that comprehensive welfare states of the Nordic model should present the smallest inequalities. This might have been true in the 1980s, or earlier (Vågerö and Eriksson 1997). Later data suggests however that this is not any more the case (Mackenbach 2008). Most west European states nowadays offer a minimum of welfare provisions and social protection. The most striking finding in the European comparative studies is therefore the divide between east and west Europe. Social inequalities in mortality are much more pronounced in the former communist countries of Easter Europe. This is both a legacy from the past and a response to the system collapse in the 1990s (Vågerö 2010).
Conclusions
People are living longer. There is a tremendous increase in life expectancy and longevity throughout much of the world. The success in reducing infant and child mortality contributes greatly to the convergence in age-at-death globally. Adult mortality trends and life expectancy demonstrate a long term convergence globally, which is broken around 1990. The divergence after that point primarily reflects developments in two regions of the world, sub-Saharan Africa and former Soviet Union. Adult mortality is strongly socially differentiated in all countries. Lower death rates have been achieved in many populations at each stage of life, with a small but growing number achieve active lives through eight and nine decades. Nevertheless, others lag behind or even experience rising mortality trends. Within the richer countries, those with more education tend to live longer than those with less education; shorter lives are more common in many of the less-developed countries, often caused by high adult mortality rates; those burdened by the HIV/AIDS pandemic, and many in post-communist Eastern Europe. While overall gains in life expectancy and longevity are substantial and promising, national and global data indicate divergence as well as convergence. Achievement of better health and more equal life spans remains a priority in the global health and development agenda.
3. Diminished health: Morbidity, disability and chronic conditions
Diminished health compromises the value of longevity: the prospect of longer lifespans has less appeal – or, in extreme cases, none at all – if those years are accompanied by poor health.
And regardless of longevity, diminished health is of concern in its own right for many reasons, including pain and discomfort, limitations or impediments to important activities, social isolation and stigma; and for occasioning the need for seeking and paying for care, which may be both urgent and financially catastrophic.
These are not merely biomedical considerations. Social acceptance can reduce or eliminate the stigma that many experience along with a diagnosis of HIV infection or cancer. Limitations on mobility, hearing and vision, and even cognitive function are much less burdensome in welcoming, tolerant social and physical environments. Serious illness does not lead to bankruptcy where there is social insurance.
A purely biomedical understanding of diminished health and disability would miss subtle but important dimensions of these issues. Dyslexia (a learning disorder consisting in a difficulty reading) is problematic in some social and natural contexts and of no importance in others, while other health conditions, such as migraine headaches, cause hardships in every context. Some health problems, such as disfigurement, limit people’s activities only because of social customs and the actions of others, while others would limit or harm people even given optimal social accommodations. Some health issues, such as the loss of an arm, provide no compensating benefits. Other problems, such as blindness, while limiting a crucial capacity, may sharpen the other senses and heighten the satisfactions individuals receive from them. There are many different ways in which humans may flourish, and health conditions that interfere with some of these ways need not prevent individuals from living well. When some activists in the Deaf community maintain that deafness is not a disability, they obviously do not mean that it does not limit a significant human capacity. Part of what they mean is that deafness need not prevent people from living well. It is important to note however that a significant proportion of people with hearing loss, particularly in low income countries, do not have access to hearing aids (Lancet, 2016; Henshaw et al, 2015).
Before discussing or assessing trends in people’s experience of diminished health, it is necessary to tackle the conceptual problem of clarifying what could be meant by “diminished health.” People speak of “morbidity,” “disability,” “impairment,” “handicap,” “injury,” “disease,” “pathology,” and “illness.” Obviously, these are not the same, and picking any term as a catch-all risks serious confusion. If, for example, one regards any diminution of health as a loss in “health-related quality of life,” as the most common generic health measurement schemes maintain, then one provokes the justified response of the Deaf community that although the lives of the deaf are different than those of people who can hear, they are of no lesser quality. A different issue arises when one considers the millions of premenstrual women who take oral contraceptives to induce infertility, which other women seek medical help to alleviate. Are the voluntarily infertile, like those who are involuntarily infertile in a diminished health state? At the same time, unlike those who have a bout of stomach flu, for example, those who are unwillingly infertile would not describe their health problem as an illness or a sickness.
Instead of conceptualizing health decrements as involving lesser health-related quality of life, one prominent group of health economists maintains that health limitations can all be conceived as limitations on activities and hence as “disabilities” of one sort of other. But this language may be just as misleading as describing health problems as diminishing quality of life. It is at the very least awkward to describe burns, rashes, and pains as disabilities. It would probably be least misleading to speak of “health decrements, limitations, or problems” but since “disability” is so widely used by demographers, epidemiologists and health economists, we shall speak of all shortfalls of health as disabilities. Still, it is important to recognize that “disability” is herein a technical term for any sort of health issue, many of which would not in everyday language be called “disabilities.”
The remarkable improvements in longevity and life expectancy documented in Section 2 do not automatically imply any diminution in disability. To the contrary, if the extension of life leaves individuals bed-ridden and suffering, then people may end up trading longer life for more years with disability. But it is important not to be misled here. Along with the health problems that come with the additional years are all the good things that those years provide. Apart from the rare cases in which the additional lifespan consists in suffering or humiliation, longer life would be a benefit.
One may question this conclusion, that longer life is usually a benefit, in two ways. First, an extended period of disability at the end of one’s life changes its overall “narrative” (Griffin 1986, Velleman, 1991). Some would argue that a long period of substantially diminished physical, cognitive, or emotional capacities decreases how well that life as a whole will have gone, compared to the life of a vigorous, competent and authoritative person that ends with no long period of dependency on others, mental confusion, or inability to contribute to the maintenance of a household. We do not take a stance on this controversial question. Second, even if a longer life is almost always a benefit to the individual, it may be costly to others. If individuals live into their nineties and retire in their sixties, then even if they do not require expensive care, they still require support from the working-age population. They may provide some compensation in the form of the wisdom and cultural continuity that they pass along, but providing for them can be a struggle, especially in societies in which there have been recent decreases in fertility and hence relatively few working age adults to support them.
3.1 Trends in disability
The data concerning trends in disability are much less clear than the data concerning trends in longevity. However, the most recent World Report on Disability provides the following data. Between 785 million (15.6% of the world population) and 975 million (19.4%) of people aged 15 years and older are estimated to live with some form of a disability. 110 million (between 11% and 14%) have significant difficulties in functioning (severe disability for conditions such as quadriplegia, severe depression, blindness). The Global Burden of Disease measures childhood (0-14 years) disabilities and estimates that 95million children (5.1%) live with disability. Of these 13 million (0.7%) have ‘severe disability’.
The number of people with disabilities is growing due to ageing and the global increase in chronic health conditions, in particular cardiovascular diseases, diabetes, neurodegenerative diseases and health disorders. Chronic diseases account for 66.5% of all years lived with disability in low and middle income countries. Conditions like diabetes are associated with physical disabilities (e.g blindness, limb amputations) and mental health disorders and neurodegenerative conditions (depression, dementia) (Leone et al, 2012). As the number of people living with co-morbid and multi-morbid conditions rise, the prevalence rates of physical disabilities and mental health disorders also rise (Barnett et al, 2012; Smith et al, 2012).
Generally the most vulnerable adult populations globally are: (1) people from the poorest wealth quintile; (2) women; (3) older people; and (4) people who are unemployed with low educational qualifications. In child and adolescent populations, groups from poorer households and from ethnic minority groups have a significantly higher risk of disability (UNCF, 2008).
Not all people with disabilities are equally disadvantaged. Women with disabilities experience gendered discrimination and stigma (Allotey and Gyapong, 2005). Children with physical impairments fare better than children with intellectual or sensory impairments at school. Among the adult population, people with mental health and intellectual impairments are more likely to be excluded from the labour market. LMICs are disproportionately affected by NCDs and the double burden of NCDs and infectious diseases especially for the poorest citizens and increasingly those in productive years under age 40) (Bukhman et al, 2015). These groups are more likely to bear a significant proportion of rising levels and cost of disabilities.
3.2 Addressing disabilities
There is a general lack of standardized culturally-sensitive data on disability. The WHO (2011, p.20) observes that “methodologies for collecting data on people with disabilities need to be developed, tested cross-culturally and applied consistently”. The data that exists suggests that people with disabilities have poorer health outcomes (e.g greater vulnerability to preventable secondary conditions, co-morbid chronic conditions and age-related conditions; higher risk of being exposed to violence), less economic partication, higher rates of poverty (a vicious cycle), increased dependency and restricted participation. Children with disabilities have lower educational achievements.
There are major differences between high income and LMICs regarding the creation of enabling environments, including implementing disability policies, and training professionals who work in rehabilitation or special education. So people with disabilities in LMICs face greater risks and poorer health and life outcomes compared to people with disabilities in high income countries.
In Ghana, for example, the prevalence of physical disability is estimated at 7-10% and the prevalence of mental health disorders is estimated at 13% (WHO, 2007). Adults and children living with disabilities do not have access to appropriate health and social care[11] and they experience stigma and associated socio-cultural responses that can be life restricting. Ghana has a disability policy and a mental health policy – both of which are informed by contemporary global discourses on disability and mental health and focus on rights-based prevention and intervention (de-Graft Aikins, 2015). However, neither policy has been fully implemented as no funds have been allocated to support governance and service delivery and inequalities in care persist especially for children, rural communities and older adults (de-Graft Aikins and Koram, In Press). Similar gaps between policy rhetoric and action relating to disability and mental health are reported in other African countries (Akyeampong et al, 2015; Faydi et al, 2011) and in low and middle income countries in other regions (Saxena et al, 2011; Prince et al, 2007).
Fundamentally, resources required to support or enhance the quality of life differ significantly within and between countries. In low income countries it is estimated that less than 5% of the disabled gain access to rehabilitative and associated services (DFID, 2010). Paraplegia in a low income country setting, for instance, could still result in a reasonable quality of life with access to a wheel chair or crutches to be used in a built urban environment to support it. Similarly, with resources to ensure activities of daily living and access to physiotherapy, function and ability to engage within the community can be enhanced. Poorer families within the same lower income country may probably not have access to wheelchairs and even if they did, may not live the built environment that would enable the adequate functioning of a wheel chair. Indeed there is evidence to suggest that life expectancy, in such settings is significantly reduced from complications of the disability that would not arise in an environment where there was access to basic rehabilitation, nursing and social care (Allotey et al, 2003; Reidpath et al, 2003). In contrast, a similar injury that results in comparable reduction in physiological function in a high income country would be provide an experience where social support and social protection, access to technology, high quality physiotherapy and rehabilitation and a disability friendly environment result in better health outcomes (Allotey et al, 2003). Participation in the Paralympics provides a stark indication of the inequalities in disability support across countries (Le Clair, 2012).
3.3 Addressing diminished health and disabilities
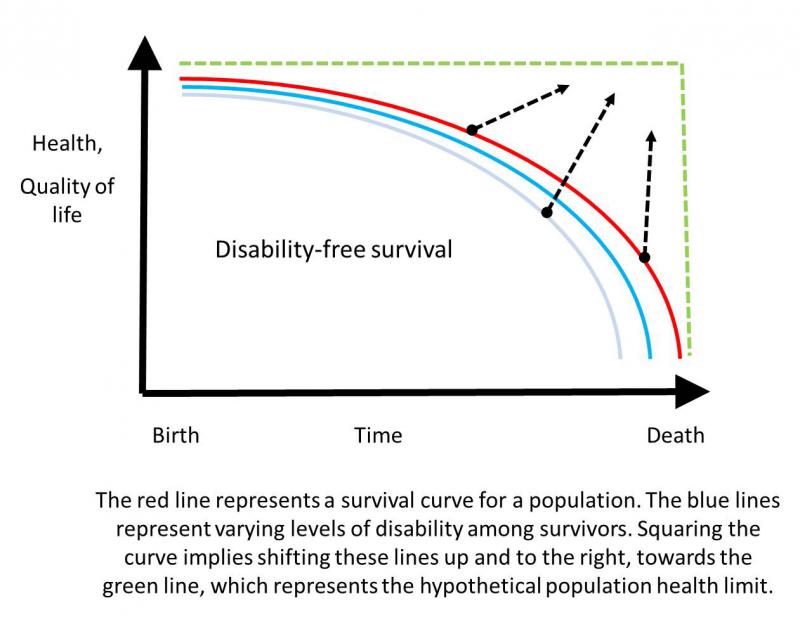
In his 1980 paper, ‘Aging, Natural Death, and the Compression of Morbidity,” James Fries sketched a health care agenda of self-evident appeal: raising the average age of first infirmity, thereby making the morbidity curve more rectangular (Fries 1980). This provides a succinct statement of the ideal: health and vigor extending as close as possible to our inevitable deaths.
(Association of Faculties of Medicine of Canada, 2009)
Whether the compression of morbidity can or will approach this theoretical limit remains uncertain. Efforts to extend the lifespan might come at the cost of adding period of morbidity – a pattern visible in the continuous progress of perinatal intensive care, where achievements in reducing the age of viability have been accompanied, at least initially, by additional disability (Brosco 2010).
Continuing progress in addressing disability, however, should not be understood in purely biomedical terms. In addition to efforts to prevent the disabling injury and morbidity, and to find and implement the means for restoring function, there remains a strong and complex social component. The disabled should be able to expect extensive accommodations in their physical and cultural environment and access to technological aids that reduce or even eliminate the associated personal burden. These range from motorized wheel chairs and alternative means of communication to building designs, education of the non-disabled public to overcome prejudice and misunderstandng, and efforts to minimize social isolation. The goal of supporting and enhancing the autonomy of those living with disabilities includes assistance in self-care, and support for communities and associations of the disabled. The latter should accept and legitimate the insistence by some disabled, such as the deaf, that their capabilities provide alternative rather than deficient patterns of functioning that may be viewed as having intrinsic value.
The disabling barriers include inadequate policies and standards; negative social and professional attitudes; lack of provision of services; problems with service delivery; inadequate funding for disability services; lack of accessibility (environmental, social, institutional); lack of consultation, involvement, participation in the formulation and implementation of policies; lack of evidence and data (WHO, 2011). Low income countries are more likely to have a higher number of disabling barriers than high income countries.
With increasing life expectancy, there is a growing need to identify and provide support for ageing and chronic disease related poor health. There remains an underlying assumption about the importance of extended family in lower income country contexts. However with the dynamism of globalization and urbanization there are growing numbers of the elderly living alone (Wan Ibrahim et al, 2012; de-Graft Aikins et al, 2016).
Conclusion
The prospect of longer lifespans will be attractive only if the added years are not seriously compromised by diminished health, disability, and chronic illness. The “squaring of the morbidity curve” remains a theoretical ideal whose prospects remain uncertain.
Disability has both biomedical and social components. What makes a condition disabling for an individual may depend on the physical environment and on social attitudes as much as, or even more than, compromised function. Support and respect for those living with disabilities requires affirmative efforts of accommodation, assistance, toleration, and respect for perspectives and priorities of “differently abled” communities.
4. Reproduction
Reproduction includes the biological processes and management of sexual practice, pregnancy, menstruation, abortion, birth, the treatment of infertility, reproductive technologies, birth control, adoption, conception, miscarriage, sterilization and menopause. It also includes the collection of vital statistics, the analysis of demographic trends, population management, the codification of the categories of maternal and infant mortality, the management of family formation, parenthood (both same-sex and heterosexual) and child-rearing. More than in any other area of global health, reproduction engenders strong views that are based on demography, politics, social values, ideology, religion and morality. The extent to which people can enjoy their sexual and reproductive health is invariably intertwined with issues of disadvantage, inequity and rights violations: encompassing gender based violence; stigmatization on the basis of sexuality; and structural and system wide barriers to accessing quality care. Who has sex, how and when they have it, whether, when and how often they reproduce, or have access to information and care for their sexual and reproductive health is in large part determined by, gender roles and power, societies, laws, politicians and increasingly, global funders (Allotey et al. 2011).
Given this chapter’s focus on how inequality shapes the changing contours of human life, we deploy “stratified reproduction”, a concept coined by the anthropologist Shellee Colen to describe “the power relations by whom some categories of people are empowered to nurture and reproduce while others are disempowered” (Colen 1995; Whittaker 2010; Ginsburg and Rapp 1995, 3). The lens of reproductive stratification demonstrates how resources and class position shape reproduction. The concept can be used in analyzing the difference in reproductive horizons of West Indian nannies and the affluent families in New York City who they work for, how IMF mandated austerity measures and structural adjustment in the developing world have exacerbated differences in global rates of maternal mortality, and in how reproductive processes align with a distinction between communities that need “productive children” who contribute to household economies and communities that cultivate “priceless” children who are to be consumed for by their parents.
4.1 Measuring reproduction
Understanding the measurement of reproduction is critical to the domains across which inequities can be assessed. Demography plays a key role where reproduction is discussed primarily in the context of its importance to ‘reproduction’ of the population and to the control of the size of the population. From a gender and rights perspective, disaggregation of the data is critical to understanding who is reproducing, at what age, how often and some measure of fertility control and choice, as a proxy indicator of inequities.
Demographers measure reproduction by a set of indicators which vary considerably in their meaning, and when interpreting time trends or differentials in reproduction, on must pay careful attention to the precise meanings of these indicators. Birth statistics usually start from the absolute counts of births that are registered in a given territory over a certain period, typically a calendar year. In countries that do not have complete vital registration systems this information is often estimated with the help of surveys. To calculate the Crude Birth Rate (often called only the Birth rate), this absolute birth count is related to the mid-year resident population in the territory under consideration. The crude birth rate can be used to compare birth intensities of different populations across time and space, but does not consider the influence of age structure.
At the aggregate level the process by which populations are renewed through the appearance of new members while older members disappear through death has also been labeled “Demographic Metabolism” (Ryder 1965) which can also be interpreted as younger generations replacing older ones. If the younger cohorts are in important ways different from previous ones this process of cohort replacement can also be seen as a force of social change that can be described mathematically and can serve as a basis for forecasting the changing composition of the population for decades into the future (Lutz 2013).
More sophisticated measures of reproduction differentiate birth by the age of mothers at the time of birth. As a convenience, maternal age rather than paternal age is almost always used, because there are always some births for which no information on the father is available and also because the reproductive age span for women is more clearly confined by physiological limits. Within this age span there are also distinct patterns of age-specific fertility rates which – depending on the overall level of fertility – tend to peak in the age groups 25-35. For this reason the age structure of any given population also has a great influence on the number of babies born. In other words, in two societies with equal numbers of children per women the crude birth rate will be higher in the population that has a high proportion of women in the prime childbearing ages. For this reason the use of age-standardized fertility rates has become the norm for comparative analyses in reproduction. Three such indicators dominate the discussions: The Total Fertility Rate (TFR) is the sum of age-specific fertility rates (all children born to women of a certain age group divided by the number of women in this age group); the Gross Reproduction Rate (GRR) is identical to the TFR except for the fact that it only considers girl babies and thus gives the average number of daughters born to women over their lives; the Net Reproduction Rate (NRR) also considers the survival of the child from birth to the mean age of childbearing and thus gives the extent to which one generation of mothers is replaced by another one. A NRR of 1.0 thus means that the following generation of women reaching reproductive age will be exactly the same as the previous one; a NRR of 2.0 means that the population doubles each generation.
Another important distinction in the measurement of reproduction is that between a period and a cohort perspective. While period rates summarize the reproductive experience of different age groups of women in one period (typically a calendar year) cohort rates describe the experience of birth cohorts of women. During times of changes in reproductive behavior, the two kinds of rates can show very different pictures. Only cohort TFRs can in a strict sense be called the mean number of children per women, which has the disadvantage that one has to wait at least until the birth cohort has reached around age 50. Period TFRs are sometimes characterized as referring to synthetic cohorts because they give the mean number of children that a hypothetical cohort of women would have that experienced all the age-specific fertility rates that are observed in one calendar year. During times of changes in the timing of births the period TFRs can be quite different from cohort TFRs, in particular during times of postponement of childbearing (measured through an increase in the mean age of childbearing), period TFRs can be artificially depressed (tempo effect). Recently, methods have been developed to estimate tempo-adjusted period TFRs that can be interpreted as the “period quantum” of fertility or the mean number of children per woman as implied by reproductive behavior in recent periods (Bongaarts and Feeney, Soptka et al). A naïve interpretation of the period TFRs as the mean number of children can lead to misleading conclusions (Sobotka and Lutz..).
4.2 Determinants of reproduction
The literature on the determinants of fertility distinguishes between proximate determinants and underlying determinants. The proximate determinants are the factors that are immediately causing pregnancy and birth in a biological sense. According to Bongaarts (1978) these determinants include the age of beginning of sexual activity and the frequency of intercourse, the prevalence and effectiveness of contraception, the prevalence of induced abortion (plus spontaneous intra-uterine mortality) and the duration of post-partum infecundity. Any change in observed fertility levels occurs through changes in one or more of these proximate determinants which explain the mechanisms but not why women and couples are changing their behaviors.
When discussing the underlying social, economic and political determinants of fertility it is useful to distinguish between the secular decline in fertility levels which is part of the demographic transition from pre-modern high to modern low levels and the variations within low fertility societies. The global fertility transition began in France in the 19th century and by the beginning of the 20th century had started in most industrialized societies. It then spread to the second half of the last century. Except for a few pockets of still very high traditional fertility levels in Africa this secular fertility transition has been completed or is under way in virtually all parts of the world. The global TFR has declined from 5.0 in 1960-65 to 2.4 in 2010-15 (United Nations Population Division 2015). But even before the onset of the demographic transition, fertility levels varied among populations due to different marriage patterns and different lengths of post-partum infecundity, which are associated with different breast-feeding patterns. In Western Europe fertility levels in the 18th century were lower than in Eastern Europe and most of the rest of the world due to a distinct “European Marriage Pattern” (Hajnal 19..) which was characterized by a rather late age at marriage and high proportions of men and women remaining unmarried. On the other hand some traditional hunter and gatherer populations show remarkably low fertility levels due to unusually long birth intervals that are associated with extended breast-feeding (Howell, 1979). But despite of these different levels of overall fertility, one finds no significant evidence of parity-specific fertility control in any of these traditional societies. There appears to have been no conscious family limitation, where the decision for an additional birth is dependent on the number of children already born to the family (Coale and Trussell 1974).
According to demographic transition theory, conscious family limitation has been a social innovation that was brought about by social and economic factors as well as cultural diffusion processes. While in traditional cultures there is evidence for some methods of avoiding pregnancies as a consequence of non-marital sex, this seems to have been largely unthinkable within marriage (van de Walle 1992). Based on an analysis of historical fertility transitions in all provinces of Europe, Ansley Coale (1973) specified a set of three pre-conditions for a lasting fertility decline: (a) Fertility must be regarded as being within the realm of conscious choice. This factor seems to be closely associated with female basic education but cultural diffusion and mass media can also play a role. (b) There must be objective advantages to lower fertility. These can range from economic factors, to urbanization to health reasons. (c) Acceptable means of fertility control must be available. What is considered as acceptable is dependent on the specific cultural context, particularly with respect to abortion. In the context of the current fertility decline in developing countries, this factor also relates directly to the availability of modern reproductive health services.
How low fertility rates will fall in the later phases of demographic transition and what differentials within and between societies will prevail are topics of intense scientific discussions. Basten, Sobotka and Zeman (2014) provide the most comprehensive recent summary of fertility trends and differentials in low fertility countries as well as the different theories, approaches and arguments that can help to explain and forecast these differentials. Fuchs and Goujon (2014) provide a comparable assessment for countries whose fertility levels are still higher (with TFRs above 2.5). These assessments are based on the input of hundreds of internal population experts and cover all world regions. They discuss the drivers of fertility in four broad domains: (1) Reproductive Health: Availability of family planning, side effects of contraceptives, traditional methods, abortion, religious attitudes to contraception, etc. ; (2) Economic costs and benefits: Child labor, cost of urban upbringing, old age security, value of education etc. ; (3) Status of women: Arranged marriage, age at marriage, female educational status, autonomous contraceptive choice, male support of contraception, female labor force participation etc.; (4) Cultural change: Ideal family size, son preference, politically promoted norms, attitude to childlessness, educational differentials etc. For the case of low fertility countries there are much more detailed analyses regarding the nature of the partner relationship as well as different forms of combining employment and family care. Given this very broad range of relevant factors determining reproduction in different societies we can in the following sections discuss only highly selected aspects.
4.3 Population Growth, Fertility Control and reproduction governance
The development of the nation state in the eighteenth, nineteenth and twentieth centuries produced a new focus on internal populations and vital statistics and the measurement of fertility. This focus codified sexuality and reproduction as processes that should be governed as a matter of great interest to the nation (Greenhalgh 2008; Tarlo 2003; Unnithan-Kumar 2004) (Morgan and Roberts 2012).
We can see this interest through the development of the legal and medical management of reproduction that sought to control reproductive behavior in both colonizing and colonized nations. Examples of these new regulatory forms include the late nineteenth century initiation of laws and morality campaigns directed towards making prostitution, abortion, and homosexuality illegal activities. Additionally, birth attendance (banning midwifery), fertility rates, infant feeding, and contraception were all newly regulated through legal, moral and medical means in the efforts to create strong working and fighting populations within nation states. Throughout the twentieth century and into the twenty-first, concerns about over and under population have been paramount in defining nations often through coercive means, such as eugenic programs or the inducement to reproduce.
With the exponential rise of world population new regulatory measures to curb overpopulation, new measures to curb population growth were instituted by nation states and international agengies, especially in the developing world. Fertility rates are highest in lower income countries in Africa and Asia. China and India now have the largest populations with the United States trailing far behind in third place. In much of the developing world, the management of reproduction during the Cold War and beyond took the form of internationally driven programs to limit and control specific populations. Deriving from early twentieth century nationalistic, eugenic policies, these programs sought to limit the population growth of developing nations to enrich their populations and make the world safe from communism. Conversely, wealthier nations in Western Europe and Japan have seen population decline often described as harbingers of national decline.
To combat this top down approach to population control, the Cairo International Conference on Population and Development in 1994 and the Fourth World Conference on Women in Beijing in 1995 developed programs of action through a human rights-based approach to reproductive health (Haberland 2002; Goldberg 2009). The approach advocated for individual rights, particularly women’s rights over fertility choices, with the underlying assumption that given that control, fertility would be curtailed. These efforts met with significant resistance, on religious and political grounds (Berer 2011). Countries like the United States placed limits on aid funding based on reproduction policies (Cohen 2003; Alvaro, Palma, and Dardet 2006). The Catholic Church also had significant influence over how reproductive rights played out in several countries. Despite these obstacles, international discussions of reproduction since Cairo have tended to be framed in terms of individual rights. Other countries developed other strategies to limit fertility, such as the one child policy in China and forced sterilizations in parts of the Americas.
30 years later, birth rates have dropped dramatically. However, reproduction and the rights-based approach remain controversial. In emphasizing rights, this approach has made it natural to conceptualize some of the issues as a competition between the ‘right-to-life’ of the unborn and the ‘reproductive rights’ of women. Control of women’s fertility has been exercised on other coercive forms in conflict situations through the use of ‘breeding programs’ (Hoile et al. 2002; Allotey and Reidpath 2015) and pressure, including through incentives, towards redistribution of resources across ethnic groups (Malaysia: Where Big Is Still Better. For Malays, Large Families Are Part of the Plan 1993)[12].
We can see the stratification at work in terms of focus on population where for instance sub-Saharan Africa the site of much global anxiety about over population is also the site of the worlds largest infertility belt due to the iatrogenic effects of poor health care infrastructure.
4.4 Abortion and contraception
The control of fertility and birth through contraception and abortion has been the most controversial aspects of reproductive policy. One explanation is that these issues place women in control of the shape of their lives and sexuality, challenging traditional female roles. Sterilization is also controversial, in part for the same reason, but also because of the coercion in forced sterilization. Modern contraceptive methods became widely available in in the early part of twentieth century and have been partially responsible in lowering fertility rates worldwide. The use of contraception and abortion are highly stratified. Even where certain means of fertility control such as abortion are illegal, women with more resources have access. Women have access to contraception in most industrialized nations and in many parts of the developing world that were considered overpopulated.
More coercive population control can be found in China, in its one child policy, in India that lowers fertility rates though giving ration cards in return for sterilization and in Tibet, Haiti, and Peru – often with groups considered unworthy of reproducing. By the eugenic logic of the earlier twentieth century, governments seek to limit the reproduction of minority groups, low castes, and indigenous communities. While development experts have understood lowered fertility rates to be key to economic development, many subaltern groups have framed population reduction policies and programs as forms of genocide.
Abortion only became became illegal from the late nineteenth century on (Mohr 1978), when states came to see robust and large populations as key to building strong nation. Illegality was framed around morality and the perceived risk of the procedure. The anthropological literature on personhood reveals North American debates about when life begins as local and specific. In different non-western sites personhood can commence at various times, often post birth; and the concept of individual life is not relevant to how children are made at all (Browner 1976; Conklin and Morgan 1996; Kaufman and Morgan 2005; Picone 1998; Tomkins et al, 2015). Even within the Catholic Church, currently one of the staunchest opponents of abortion, the definition of beginnings of life have changed over time.
As many scholars and activists have demonstrated, illegality and censure does not prevent the practice of abortion. Despite the continued illegality of on-demand abortion in Latin America, except in Cuba and now Mexico City, it now has some of the highest abortion rates in the world (Browner 1979; Htun 2003; Scrimshaw 1985). In these nations women with means can access safe abortion, while women without means cannot. Abortion conducted with trained practitioners and under sterile medical conditions is extremely safe, safer than carrying a child to term. Of the 42 million abortions performed each year 20 million are unsafe. Of these 20 million about 18.5 take place in developing nations About 68,000 women die each year from complications due to unsafe abortion annually, 13% of maternal mortality deaths[13].
Gender based mobilization for the right to abortion has been variable. In Latin America for instance, it has been hampered because unlike the right to vote – abortions illegality affects women differentially by class. Clandestine abortion is easily available and relatively safe for women with means, thus there has been little impetus to work toward legalization (Htun 2003;)(Mooney 2009, 51). The current model for abortion decriminalization in developing countries makes the case for the right to public health, rather than the North American “right to choose” (Morgan and Roberts 2009, 2011).
Medical abortion, (pharmaceutically induced) abortion is changing the abortion landscape by providing women a safe and discrete means to abort outside of clinical settings. Reproductive stratification is also evident in access to medical abortion given that the ideal method involves a combination of mifepristone and misoprostol which achieves the highest efficacy with the fewest side effects. In many regions of the world, only mifepristone is available[14].
4.5 Assisted reproductive technologies and selective reproductive technologies[15]
The late twentieth century saw the rapid development of assisted reproductive technologies that facilitate fertility and selective reproductive technologies that facilitate and prevent the births of children who for one reason or another are not wanted. As several social scientists and scholars of the social studies of science have argued, reproduction has always been assisted and children have always selected through various kinds of social arrangements and practices, as well as familiar technologies of infant formula, paper work and forceps. The availability and reach of assistance and selection has, however, never been greater. This availability falls along stratified lines.
We can see stratification at work in the development and use of assisted reproductive technologies and selective reproductive technologies around the world. In the developed world, assisted reproductive technologies, such as in vitro fertilization, intracytoplasmic sperm injection (ICSI), egg donation and surrogate motherhood have produced anxieties about interference with nature. In the developing world assisted reproduction is now geared towards combatting iatrogenic infertility – which perhaps involves ignoring larger structural causes for the high rates in these areas.
Rather than aiming to overcome infertility, selective reproductive technologies are used to determine which children are born. Two of the most common purposes are sex selection and preventing the birth of children with certain developmental conditions. In commercial societies with extensive public pre-natal programs fewer and fewer children are born with conditions such as Down’s syndrome. Disability rights advocates criticize this as an injustice, while defenders point to the difference between choosing not to bring someone with disabilities into existence and violating the rights of or showing disrespect to those who have disabilities.
In many developing countries the private use of selective technologies like amniocenteses and pre-implantation genetic diagnoses has resulted in a skewed sex ratio in favor of boys. This form of sex selection is explained by the fact that in the past, extended families have prospered through the propagation of boys. In fact in some places such as Ghana, women who only have daughters are considered infertile because she has not produced what is necessary for family continuity.
4.6 Family composition
While reproduction seems to reside in individual families in Western Europe and North America, reproduction is often organized as explicitly collective in non-industrialized locations, whether on the scale of the extended family, village, community, region or nation.
The comparative examination of adoption and child circulation has contributed to insights into the Eurocentric privileging of intergenerational bio-genetic ties, where as the circulation of children often reinforces material care relations between a larger group of adults as much as the reproduction of children (Leifsen 2010; Leinaweaver 2008; Modell 1995). Chapter 17, in this global report, offers a more comprehensive discussion on this theme.
4.7 Developmental and Environmental Approaches to Reproduction
Within Euro-American contexts, the early twentieth century saw the rise of the theory that mothers can do almost nothing to harm a fetus in utero, based on the assumption that the placenta was a “perfect barrier” between the two. This separation of the mother from her offspring was supported through the growing consensus about genetic heritability. In much of Western Europe and North America, scientists posited genes as determinative of much of phenotype and behavior, a framework that came to be the predominate model by the late twentieth century. Genetic determinism was predicated on a sense of DNA as a book transmitting building instructions across generations unchanged by the material, economic, or political environment. However, with the completion of the Human Genome Project in 2003, scientists found that DNA provides fewer instructions for cell expression than predicted and the search began for other mechanisms that contribute to biological existence. In the last two decades emerging developmental and environmental models for human health predict that the conditions under which people are born play a much larger role in shaping later life well being than thought previously.
One site where environment seems to be of particular importance is gestation. Epigenetic researchers examine environmentally triggered mechanisms (e.g. DNA methylation, histone modifications and DNA-binding proteins) that affect and regulate gene expression. Epigenetic researchers broadly define environment in terms of climate, stress and nutrition, emphasizing particular environmentally plastic reproductive moments such as embryogenesis, early gestation and the neonate period. Thus the bulk of epigenetic research focuses on the effects of the maternal body and maternal behavior on the “fetal programming” of offspring. Thus, as discussed in section 1, researchers have shown that children born to women stressed or starved during wartime have much higher levels of adulthood disease and lower educational attainment, characteristics that might be passed on to their children.
Epigenetics and the many empirical studies of the social determinants of health have the potential to reshape social welfare policy towards more collective and distributed action, enlisting broader support for environmental regulation, public education and health care. But within current neoliberal economic regimes in the United States and Western Europe, epigenetics researchers have focused on the implications of their findings for the behavior of pregnant women. Thus, for example, David Barker, one of the main popularizes of the concept of “fetal programming” and the “developmental origin of adult disease hypothesis” DOADh argues that “research should be redirected towards the intrauterine environment rather than the environment in later childhood such as housing, family, income, diet and other influences” (Barker 1990).
Similarly, governments and NGOS in developing nations find it more feasible to fund programs targeting pregnant women and infants than restructuring decayed public institutions such as schools and health care facilities. Pharmaceutical companies are attempting to produce drugs that will activate epigenetic mechanisms. One drug under research seeks to calm children who experienced “bad mothering” in the neonate period. Such a drug obviously does nothing to address the larger (and from the perspective of a pharmaceutical company, profitless) political and economic factors that produced “bad mothers” to begin with. The targets of these discussions and interventions are women of reproductive age, made yet again, to bear the bulk of responsibility for how their offspring fare. Epigenetics and DOADh might reshape our understanding of socio-biological existences, or they might instead reinforce the policing of the behavior of pregnant women.
A developmental/environmental approach has started to shift the focus of reproductive policy towards more general environmental factors. Declines in human male sperm production and the falling age of female menstruation worldwide have been linked to factors ranging from increased nutrition to synthetic chemical compounds like endocrine disruptors, BPA thaltes and antibiotics, and growth hormones (Steingraber, 2007).
This environmental approach also allows social and biological scientists to shift the focus away from the individual reproductive body to larger global environmental conditions that shape reproduction in disparate and stratified ways. The historian of science Michelle Murphy argues that if we ask, “Where does biological reproduction reside?” the answer “the body” is simply not up to the task (Murphy 2011). Murphy advances a framework of “distributed reproduction” that allows us to examine “what counts as biological reproduction by tracking the dispersion of sexed living beings into their infrastructural and political economic milieu” (Murphy 2011, 22). The notion of the individual body is not up to the task, for instance, of understanding how only 35 boys are born for every 100 girls among the First Nations Aamjiwnaang peoples in Eastern Canada, where, in the local waterways, the gonads and sex ratios of fish, fowl and reptiles have also been dramatically altered (Murphy 2013). To grasp the determinants of reproduction, Murphy argues that we need to move beyond individual bodies and sort through the specific tangles of diverse causal factors affecting people and fish.
Conclusion
Reproduction differs with culture and social and income class, and it is affected by a society’s health infrastructure.
5. Enhancement: Better than well
This section will explore the possible implications of human enhancement interventions, present and future, on the limits of healthcare and the fair distribution of medical resources. We shall suggest that many expectation and concerns regarding the biological transformation of humans by radical enhancement may be exaggerated. Rather, the important changes in the human condition that human enhancement is likely to bring about will be social and cultural and mediated through the social effects, sometimes subtle, of the widespread adoption of such practices. Still, these changes will require regulation and rethinking of long-established principles in health policy.
5.1 What is enhancement?
A number of drugs that are usually considered as human enhancements are in use today. Examples are performance enhancing drugs in sports, off-label use of stimulants but also everyday products such as coffee. Among bioethicists, human enhancement is usually understood as a biomedical intervention that is used to improve human biological functioning beyond what is necessary to restore or sustain health (Juengst and Moseley 2016). This notion is contrasted with treatment, which is understood as a biomedical intervention that restores or sustains health. However, the same drug or procedure can sometimes be used both to treat ill health and to enhance humans. For example, the drug Modafinil is routinely used as a treatment for disorders such as narcolepsy and would in this case not be considered an enhancement. However, this drug is also used as a human enhancement by (among others) the United States Air force to enhance wakefulness in pilots during extended air missions.[16]
We may also distinguish between radical and non-radical enhancement. An intervention is a radical enhancement if it improves a human function such that it surpasses the human range. For example, a medical treatment that would extend a person’s lifespan to 150 years would be a radical enhancement. By contrast, non-radical enhancement includes interventions that leave the improved person with abilities well within the human range. As most current and emerging human technologies belong to the latter group, our focus will be on non-radical enhancement (henceforth “enhancement”).
According to the standard definition, human enhancement is distinct from interventions that impair or don’t improve human biological functioning, such as tattoos, piercing, genital cutting, cosmetic surgery and other body modifications. We face here an interesting complication with the standard definition since some body modifications impair body functioning but confer a social advantage in some contexts. For example, skin bleaching is sometimes toxic and arguably harms the biological function of the skin (Olumide et al 2008). However, this practice would hardly be so popular if it didn’t improve the social prospects of its users. In a number of countries, lighter skin improves job prospects, wages and other social goods (ref). Thus, how improvement should be characterized with regards to human enhancement is not straightforward. Since the distinction between health related and social improvements are (sometimes) difficult to maintain, and often reinforce each other, this makes the standard definition (where functioning is understood as biological form) too narrow.
Secondly, the standard definition of enhancement as an intervention that improves a human function beyond what is necessary to restore or sustain health depends crucially on what can be considered as “health”, a notion that is highly context sensitive. For example, with modern expectations on dental health, fluoride therapy is hardly seen as an enhancement. Yet before this practice was routine, poor teeth quality was not considered to be a sign of poor health, but rather as a normal state associated with advanced age (ref). What should be considered a healthy body has differed widely across time and place, and involves a normative element. The distinction between human enhancement and medical treatment often involves evaluative or normative claims regarding which interventions that are justifiably regarded as medical treatments or which functional states that are pathological, on the one hand, and healthy or normal, on the other hand. Thus, human enhancement is not merely a descriptive concept for a set of interventions but includes both evaluative and descriptive elements [ref Williams?]. For example, sometimes when people claim that an intervention is an instance of human enhancement rather than a medical treatment, it involves an evaluative claim to the effect that the intervention under discussion is of less importance or should not be subsidised by the taxpayers.
Thirdly, whether an intervention is considered to be an enhancement also depends on what is perceived to be part of a person’s abilities rather than something the person is able to do with help of technologies external to the person. For instance, writing down some fact in a notebook and forgetting it does not seem to count as remembering that information in a notebook. Enhancement technologies are often seen as artefacts that are to a certain degree integrated with the person. According to this view, only modifications that are physically integrated with the body counts. An example of this would be performance enhancing stimulants. The account of enhancement technologies as necessarily attached or integrated with the body is complicated by the view of cognition as essentially embodied and extended (Clarke 2007). If a person’s cognitive processes are regulated and (partially) executed by its environment, why should things such as calculators, maps, whiteboards, etc., not be considered to be enhancements?
Despite these problems with the standard definition of human enhancement its use is so established that we cannot disregard it in our discussions.
< >Enhancement and priority in healthcare
While most accept that human enhancement is in at least some instances permissible, there remains considerable controversy with regards to how such interventions should be prioritized when distributing health care resources. Modern medical practice and health care policy-making faces an increasing number of conditions that could be addressed through medical interventions. A general principle that is often, implicitly or explicitly, used to guide deliberations in the face of this challenge is the idea that conditions that qualify as diseases (i.e. that impair health) yield a claim to medical resources. Let’s call this principle “Disease Priority”. A strong version of this principle states that medical interventions that do not restore or sustain health are morally wrong (Sandel 2004).[17] A weaker version of Disease Priority states that all interventions that treat or prevent disease are to be prioritized before all other interventions. This weaker notion is part of the standard approach to prioritization in the healthcare system. For example, the National Board of Health and Welfare in Sweden explicitly states that medical services not associated with disease or harm has the lowest priority in respect to the distribution of medical resources (Larsson 2007).[18]
According to Disease Priority, enhancement interventions, as we have characterised them above, would either be either morally impermissible or in the lowest priority group. However, although Disease Priority may sound plausible, it is in conflict with some instances of standard medical practice. Unwanted pregnancies, for instance, are generally considered to be a medical problem that ought to be addressed by the healthcare system, even though being pregnant or fertile is not a disease.
An alternative, more pragmatic, approach to the distribution of healthcare resources would, rather than relying on the enhancement/treatment distinction, extend medical interventions to new areas, depending on considerations such as cost, effectiveness, and equality. For example it may now (or in the near future) be possible to partly address some social problems with modern medicine. According to a new study in the New England Journal of Medicine, the medication with methylphenidate (a stimulant) of prison inmates diagnosed with ADHD seems to have led to a reduction in reoffending (Lichtenstein et al. 2012). The same medication seems to improve math and reading skills among students with ADHD, according to a study in the Journal of Pediatrics (Scheffler et al. 2009). Still, there is disagreement regarding whether ADHD is a genuine disease (Greenberg 2010). The pragmatic approach suggested here bypasses this problem and instead shifts the focus to whether the symptoms typically associated with ADHD can be effectively addressed with medical interventions at a reasonable cost, and whether it would be desirable to do so. This approach suggests that in a wide variety of contexts, social problems may be partially addressed by medical interventions. Whether or not these conditions yield a claim to medical resources should arguably depend on the safety, cost and direct and indirect effects, of the intervention and not on whether the conditions qualify as diseases. In other words, whether or not interventions that are thought of as human enhancements should have priority over interventions that sustain or restore health cannot be answered before we know the consequences of such interventions, which may vary greatly.
5.3 The limits of human enhancement
In general, known human enhancement interventions have limited medical benefits compared with many medical treatments. Sometimes human enhancements are biologically harmful or neutral but may provide a social benefit. The pragmatic outlook proposed here suggests that not only medical benefits are worth taking into consideration when assessing the relative importance of a specific intervention. For example, contraceptives have in most cases insignificant medical net benefits but have quite substantial social benefits, such as increased female workplace participation and reproductive autonomy. Some of the social effects of such interventions may not always be apparent locally, but could in the aggregate be quite significant, and this needs also to be considered. For example, we may hypothesize that if a large fraction of children would receive medication for certain behavioural traits, and this intervention was effective, then we should expect this to have significant consequences on youth culture and social norms. Nick Bostrom has noted that macroeconomic gains from increased cognitive function due to the removal of lead in gasoline have been considerable (Bostrom & Roache 2009). Similar gains could be the result of the proliferation of cognition-enhancing drugs, even when the effect of such drugs would be imperceptible on the individual level. For example, if a larger subset of the population would acquire better reading skills, this may improve the general public’s understanding of scientific concepts that are today largely unknown for most people, such as the difference between correlation and causation. Such understanding could in turn have important consequences for the future of political discourse.
However, what can be said of existing human enhancement interventions is that they are in general much less effective in improving biological functions than treatments are. Restoring human functions that have been impaired by disease is typically more effective than improving the functions of a healthy body. For example, fortifying food with essential micronutrients such as iodine to address iodine deficiency (not an enhancement, as defined here) is a much more effective way to improve intelligence (in those with said deficiency) than any existing or hypothetical cognitive enhancer.
The apparent difficulty of radically enhancing a bodily function is in most cases explained by the fact that human bodies are complex systems where different subsystems coexist in an equilibrium, where improving one function over a certain baseline often means reducing the functioning of some other functions. For example, while caffeine improves some cognitive functions, such as alertness and wakefulness, it has a detrimental effect on other functions, such emotional stability (Vilarim et al 2011). Therefore, using the enhancement/treatment distinction could in some circumstances, where enhancement and treatment compete for the same resources, be a plausible heuristic to assess the medical effectiveness of an intervention.
Moreover, any discussion of how to, from a policy-maker’s perspective, allocate medical resources should make a distinction between human enhancements that confer a positional and a non-positional advantage. The enhancement of executive functions (self-control, planning, and concentration) is for example better for the enhanced individual because such functions are very helpful in avoiding costly mistakes. The same enhancement may also confer a positional advantage, in that the person may benefit from being better than others with respect to these abilities, but it would still be good for the individual even without such a positional advantage. Other enhancements, such as cosmetic surgery or doping in elite sports, typically only confers a positional advantage. Such enhancements are only beneficial to the individual if it improves a specific function in comparison to other people. Were everyone to use the same performance-enhancing drug in a contest, then no one would be better off, and considering the side-effects, all would probably be worse off. While individuals cannot be expected to adapt their behaviour in these collective action situations, regulators should consider these problems when making decisions with regards to the allocation of medical resources. This is a typical collective action problem, where a number of individuals stand to gain from a course of action, while the same action would imply a net loss if collectively adopted. These situations need the intervention of an external actor (a regulator, for example) which can impose costs for taking such actions, thereby aligning the individual and the collective interest.
5.4 Enhancement and fairness
The world’s resources are dramatically unequally distributed, and this inequality has significant effects on human health, well-being and life prospects. Lack of access to clean water, vaccines and other crucial resources not only kill, they also stunt physical and cognitive development. For people that live under these conditions, non-enhancement interventions are likely to play a much larger role in improving their lives. Granting equal access to nutritious food, clean water, education, and other basic goods is both cheaper and more likely to make an impact than any human enhancement technology.
Yet when it comes to human functioning and biological opportunities, humans are to a large extent born equal, when their most basic needs have been met. Some opponents of human enhancement fear that this may no longer be true. The worrying prospect is that human enhancement would create a cognitive elite, that not only has superior material resources to perpetuate inequality, but who also are genetically or biologically superior to the poor (Sandel 2004; Fukuyama 2004; Habermas 200X). While this scenario is indeed disturbing, it may be less plausible than is typically assumed.
Firstly, just as non-enhancement interventions which improve cognitive ability have declining marginal impact, so do most known enhancements (Ileva 2015 [dubbelkolla]). In other words, human enhancement interventions typically improve function most in individuals whose functions are on the lower end of what can be expected from healthy individuals. For example, methylphenidate, a stimulant used to treat ADHD, seems to have a limited effect on “normal” people, but seems to have an effect among ADHD-patients that is proportional to the deficiency in attention.
Genetic selection for increased cognitive ability is also likely to follow a similar pattern. The number of genes associated with intelligence is very large, and since each gene that can improve an average person's intelligence has only a very small effect, selecting for very intelligent offspring is rarely feasible (Bostrom & Shulman 2014). However, a number of genes are known to cause mental impairment and these genes have a comparatively large effect, and could feasibly be selected against. This pattern applies to most existing human enhancement interventions.
Secondly, detractors of human enhancement typically assume that such interventions are likely to be expensive. This largely depends on what kind of intervention one considers. The price of a drug is generally speaking a function of the costs of research and testing, and the number of potential consumers. A drug that improves cognition in the general population would have a very large pool of potential consumers, and could therefore be quite cheap. If such drugs are effective, and positive externalities are quite considerable, as suggested by Bostrom, it would be an appealing option for policy makers to subsidize them. Other potential interventions are potentially much more expensive. For example, if transcranial direct current stimulation, a technique whose proponents suggest that it could enhance learning, would be as effective as claimed, this would be a technology that would be more expensive to produce and administer in scale (Kadosh et al. 2012).
This prospect, of human enhancement reinforcing prevailing inequalities, while still speculative, raises the need to address the risks of unequal access to human enhancement from a health policy perspective. If some human enhancement interventions yield a considerable advantage, policy-makers should either ensure that access to such interventions is universal or that its use is regulated. Under current policy paradigms, where off-label use of stimulants is widespread in academia (ref), the poor and disadvantaged are likely to suffer the consequences.
On a global perspective, while human enhancement is not likely to aggravate inequality more than existing health inequalities between individuals, the aggregate social effects, as described above, of some communities having access to human enhancement before other communities could have considerable effects in increasing inequalities between these communities.
5.5 Conclusions
Interventions referred to as human enhancements have become increasingly prevalent and accessible. This section has discussed a number of considerations that are relevant for policy maker that focus on problems and considerations that are present rather than science-fiction inspired speculations of potential future radical enhancement.
6. Death and dying
This section focuses on how inequality shapes death throughout the world, in terms of what we die of, how we die and our ideals for a good death. The global health agenda of a “good death” – dying of a non-communicable disease at advanced age, might seem attainable given that for the first time in history people over the age of 65 will soon outnumber children under the age of five (Ref). In keeping with the chapter’s theme of inequality however, it should be no surprise that this “good death” is far from the reality for most of the world’s people, not only in poor nations, but also amongst the poor in higher income countries (Toprani, Li, and Hadler 2016). Additionally, the goal of a universal template for a good death is in itself contestable, given dramatic variation in what constitutes a good death around the world (Russell 2015).
Anthropologists have pointed out that in many communities an ideal death “occurs after a long and successful life, at home, without violence or pain, with the dying person being at peace with his (sic) environment and having at least some control over events (Seale & Van der Geest 2004: 885)”. While the broad strokes of an ideal death might be widely shared its particulars vary widely. Thus, while in Ghana a good death is attained through “a well-organized and well-attended (public) funeral”, which expends resources in maintaining ongoing relationships, in the Netherlands a good death takes place in the period before death and the act of dying of the individual (Seale & Van der Geest 2004). These differences might be glossed as “cultural”, however, rather than culture, our focus in this section is on how inequality in regards to access to resources shapes death and dying. One problem with a cultural analysis is that despite biomedicine’s roots in specific Christian/Cartesian logics that separate mind from body (Langford 2016), bio-medicine and biological states are imagined as culture free, while death and dying that diverge from bio-medical norms are portrayed as cultural (Gordon 1988).
Additionally, cultural analysis can obscure inequality in understanding how we die. This obfuscation, can be seen in how media and “experts” problematically deploy culture in explaining practices around death. During the 2014/2015 Ebola outbreak mainstream press accounts focused on how African religious beliefs and customs, like touching the dead in order to become ancestors, or the female sharing of veils in Christian congregations served to spread Ebola in Liberia and Sierra Leone (Grundy 2014; Mark 2014). This narrative about cultural attitudes towards death obscured the fact that years of structural adjustment policies demanding social welfare austerity had stripped the region of the infrastructural supports needed to follow quarantine protocols (Robinson and Pfeiffer 2015; Nyarko et al, 2015).
According to politicians, doctors and clergy in Egypt in the early 2000’s, low rates of organ donation were due to Egyptian’s culturally backward, religious beliefs about death and the afterlife. Rates of organ donation picked up, though, through and after the Arab Spring stemming from a realigned relationship of trust between subjects and the state, after years of corruption and poor medical care. Low organ donation rates had little to do with cultural beliefs about death (Hamdy 2016). Death and dying as well as bio-medicine can be analyzed then, as phenomena shaped through history and political economic realties that often produce inequality (Lock and Gordon 1988; Singer and Baer 1995). We focus on four key themes relating to the complexity of death and dying in the global context: (1) Dying unequally; (2) Palliative care; (3) Assisted dying; and (4) New technologies of death and dying.
6.1 Dying unequally
The last century saw huge transformations in what people die of and how they die. In developed nations, people are living longer lives, with few mortalities resulting from communicable or infectious diseases (see section 2). With longevity, comes chronic conditions and complex diseases of aging that are costly to manage, e.g., more people living with heart disease, rather than dying of a heart attack. These transformations in cause of death will radically reshape how people die, where, with whom, and under what emotional and physical circumstances. Key to this transformation is the fact that in poor nations, non-communicable causes of death are usually multi-factorial, stemming from multi-level, multi-faceted largely structural causes including poverty, lack of access to healthcare, weak health systems and policy (Bukhman et al, 2015; de-Graft Aikins and Agyemang, 2016).
World-wide major causes of death are reviewed extensively in Section One, thus in this section we focus how inequality produces death and dying far from the global health ideal of a “good death.” The conditions surrounding infant and child mortality, maternal mortality, violent death, suicide, death from natural disaster and what we call “death by modernity” all highlight this inequality and shape the experience of death dramatically.
6.1.1 Infant and Child Mortality
The contrast between high and low rates of infant and child mortality plays a large part in the attribution of personhood. In contexts with high rates of infant and child mortality, personhood tends to be bestowed over time, sometimes at a child’s first or even fifth birthday, instead of at birth (Morgan 1989; Scheper-Hughes 1992). Gradual personhood is shaped within unstable life conditions where it is not likely that any one child with live to a year. These practices of gradual personhood contrast sharply with how child, infant and even “prenatal” death are marked earlier and earlier in wealthier countries, through funerals, and other forms of memorialization, as infant and child death becomes more rare and fetal personhood is further instantiated through new visualizing technologies like ultrasounds and amniocentesis (Georges 1996; Layne 2003; Taylor, Layne, and Wozniak 2004).
6.1.2 Maternal mortality
A contributing factor to maternal mortality rates in some areas of the world, comes from long-term distrust rural peoples have of state provided maternity and obstetric services. In UP, India for instance, rural people report that poverty coupled with financial extortion, rude and negligent service, and a history of coercive family planning policies keep pregnant women who might need obstetric care out of clinics and hospitals (de Kok et al, 2010).
6.1.3 Violent Death
While violent death does not make it on the top ten list of cause of death world wide it tends to be considered one of worst ways to die, and the most traumatizing for the bereaved. Violent death occurs disproportionally within poor and marginalized groups around the world. Nations in Central American have the highest country-wide rates of violent death in the world. El Savador leads with 93.09 violent deaths per thousand and and Guatemala is number two with 70. 66 deaths per thousand. In the United States homicide is the highest cause of death among black men 15-44, and African Americans are almost eight times as likely as white ones to be homicide victims.
For the bereaved, grief from the violent death of a loved one leaves behind a sense of insecurity and senselessness of the world depending on who and how the violence was committed, and whether the violent death can be commemorated (Thompson, Norris and Ruback, 1998). Comparative distress levels of inner-city family members of homicide victims. War time death complicates this picture given that in many nationalistic contexts dead warriors are considered heroes, which can serve to comfort the bereaved (refs).
6.1.4 Suicide
With its seeming random individuality, suicide was on of the first puzzles social science grappled with in delineating a social approach to problems of the modern world, shaped through the imperative to maintain robust national populations in the name of “life itself” (Durkheim 1897; Foucault 1990). While suicide can seem puzzling and pointless or even immoral from a modern global health perspective, it has been used and still is used to communicate sacrifice, honor or political resistance within collective life, which can then be celebrated and admired, especially when death is not experienced as completely disconnecting the dead from the living (Asad 2007; Staples and Widger 2012). The modern puzzlement about suicide has recently turned to alarm given that suicide rates have increased worldwide by 60 percent over the last 45 years, making it now the #15 leading cause of death, with over 75% of global suicide occurred in low- and middle-income countries in 2012. Among 15-29 year olds suicide is now the highest cause of death (WHO, 2014). As a nation, Guyana has the highest rates of suicide, with 44.4 deaths per thousand with South Korea at 28.9 per thousand at number 2. Eight Eastern European nations are represented in the top 25. lf we look at groups within nations however, the highest suicide rates in the world exist among first nations peoples in the Americas, where loss of life ways, and inter-generational continuity, poverty and violence and dispersed settlement patterns, contribute to high rates of suicide. In Nunavut, the mostly Inuit province of Canada, suicide is cause of 27% of all deaths.
State and NGO interventions have been implemented at population, sub-population and individual levels to prevent suicide and suicide attempts among these groups. Much of this attention is medicalizing, geared toward improving mental health within individuals instead of focusing on larger structural issues that shape the often, bleak collective life conditions for communities most affected by suicide (Stevenson 2014). A critical question for global health then is what suicide prevention is meant to do; save individual lives or create more equitable conditions that make life worth living?
6.1.5 Disaster
Recent key social science insights into disasters, designated natural or otherwise, demonstrates how human action, social organization and stratification shapes their occurrence and who dies in tsunamis, earthquakes floods, hurricanes heat waves, droughts and famines. As it stands, 56% of disasters happen in high income countries, while these same countries only experience 32% of the lives lost related to disaster, while low income nations experience 44% of the disasters but experienced 68% of the deaths from disaster (CRED, 2015). The psychic toll can be long term for disasters survivors when whole communities and life ways are obliterated in short order. Economic stratification then is the key determinant of mortality in disaster.
Heat waves are exemplary of how inequality shapes the death toll in disasters. With the increase in elderly people living alone, the degradation of shared urban space, and increased temperatures from global warming in the late 20th and early twenty first century, there has been a massive upswing in the rate of heat related death among the elderly. In 2003 over 11,000 people died in France during a heat wave, most of them elderly and low income and in Chicago in 1995 over 800 people died, mostly elderly poor residents living alone in dangerous urban neighborhoods, who could not afford air conditioning. They had no place to go for heat relief (Klinenberg 2002).
6.1.6 Death in an unequal modernity
There are some forms of death that are new to modernity, where infant mortality rates are lower and many conditions are more treatable. The conditions that come along with conditions affect the poor more than the wealthy. Ageing, disability, chronic diseases, mental health disorders highlight the complex burdens experienced by the world's poorest. The roots of the problem are largely structural - poverty, lack of access to healthcare, weak health systems and policy, and the industrial food systems that create unequal access to healthy food (Lang and Heasman 2016; Laudan 2015). These structural drivers condition the normalization of early death in many poor communities.
Diabetes exemplifies these issues of the unequal distribution of death by modernity, working though a double burden of over-nutrition and under-nutrition. 80% of the disease occurs in low and middle-income countries.
Mexico and Native American communities in the United Sates are a case in point for the ubiquity of diabetes. After vast changes in the post-NAFTA, Mexican food landscape, where soda and other junk food have been made cheap, sometimes cheaper than water, diabetes along with heart disease is now the top cause of death (70,000 a year). These deaths disproportionally fall among low-income people. We can also see extremely high death rates from diabetes among First Nations people in the United States who have experienced water dispossession. The Pima Tribe in the United States Southwest now have the highest rates of diabetes in the world. There was no reported incidence of diabetes before the damning of the Gila River in 1928 to facilitate the expansion of Arizona urban populations, cutting of all water to Pima farmlands. The Pima entered a period of famine, alleviated by US commodity foods like white flour and sugar, which became main diet staples (Bogardus, 1993). At this point death through diabetes is considered a societal genocide by the Pima.
6.2 Quality of Death- Palliative Care and Hospice
“Quality of life” indexes have paved the way for discussions around “quality of death”, which are measured through access to palliative and hospice care. Palliative care is now considered part of the right to health, defined by WHO as “an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering. ” (ref) Essential medicines for palliative care were included in the 18th WHO Essential Medicines List in 2013, and in May, 2014, the World Health Assembly (WHA) passed a landmark resolution urging member states to support access to essential medicines, and to strengthen palliative care as an integrated component of universal health coverage throughout the life course, stating that palliative care is an ethical responsibility of health systems (ref).
Access to palliative care however is unequally distributed and has been largely absent from the global health dialogue and consequently a low priority for donor investment (Powell et al, 2015). “In many parts of the world, hospice and palliative care is either non-existent or in its infancy, with about 5bn people living in countries with insufficient no access to medications to control severe or moderate pain”, according to the WHO. Meanwhile, in developed countries, medical services have all too often focused on preventing death rather than helping people meet death without suffering pain, discomfort and stress.” (ref)
A key assumption underlying “quality of death” is that cause of death will be a single, non-communicable disease, like cancer or heart disease hopefully at the end of life that can be palliated through the care of symptoms. Death from a single non-communicable disease disproportionality occurs in high-income nations, where resources exist for both early disease diagnosis and the end of life palliation of pain. This assumption is problematic though taking into account how there is now an ever-increasing burden of intertwined chronic and non-communicable disease in low-income nations. HIV/AIDS, diabetes, and neurodegenerative diseases present an enormous need for palliative care in low-income countries and populations, and cancer is a growing cause of death in low-income countries (de-Graft Aikins and Agyemang, 2016). In low-income countries, late diagnosis and lack of resources for palliative care make death by non-communicable disease in these nations a horrifying experience for the dying and their families (Livingston 2012). Furthermore, pain control is essential but largely unavailable in low-income countries even in cases of severe injury, acute infections, and epidemics (eg, Ebola) and the fallout of natural disasters, in which cases often end in death. Despite this widespread need, only 20 nations in total (8·5%) have integrated palliative care adequately into their health-care system.
Most studies associate palliative care with less health spending. “By increasing the proportion of community and homecare, palliative care can reduce costs associated with hospital stays and emergency admissions. In Spain, one study found that in 2006 a shift away from the use of conventional hospital treatment towards palliative care, an increase in homecare and lower use of emergency rooms generated savings of 61% compared with expenditure recorded in a 1992 study. However, the costs associated with non-cancer palliative care are higher than for cancer-related care. And as the population ages, more end- of-life care will be needed overall” (Economist report). While the utilization of both hospital-based and in-home hospice and palliative care services significantly reduced the cost of care, while providing equal if not better quality care, studies to date are primarily from developed countries. Additionally, any measurement of the true cost of palliative care would need to take into account that most of the innovative palliative care programs in low income nations are resourced in this post-structural adjustment period through a patchwork of NGO’s and the harnessing of volunteers, obscuring much of the labor costs involved in providing this kind of care, and making expenditures hard to measure (Global Atlas).
The hospice movement, advocating for end of life care at home or a home like setting, developed in the UK, which is the highest ranking nation in Quality of End-of-Life Care sub-category, which includes indicators such as public awareness, training availability, access to pain killers and doctor- patient transparency. Many wealthy nations do not come near this rating however because of poor resource allocation and policy coordination, and a focus on “strong hospital medical-care programs that see little value in hospices” and instead value the services of oncologists and “the power of medicine” (ref). For instance, hospice care in the US is available, but is only covered by health insurance if the patient is declared terminal which narrows the scope of who it can serves and which discourages its use given the US focus on heroic measures. Within this context moving to hospice care can seem like “giving up”.
We don’t necessarily have to understand “giving up” as a cultural belief that can be alleviated through the right education, but instead can link this sense to the current healthcare system in the US which rewards medical providers for procedures rather than outcomes and where hospices are paid on a daily basis, usually regardless of length of care. As more and more people spend longer living with chronic illness, the challenge will be to come up with payment models that allow for hospice care at an earlier stage, which could reduce the inevitability of heroic measures, and the sense, that hospice involves “giving up”.
One barrier to palliative care around the world is unequal access to opioids for pain relief either through lack of resources or through strict narcotics control which contributes to acute suffering in the dying (Stonington 2015). In India, one of the largest producers of opium and morphine, access by the poor to end of life pain relief is minimal because complicated regulations put in place by the British in the 19th century to control their opiate supply for export (ref). Kerala, a state with a long history of community organizing and high literacy rates, has bucked this trend through the development of comprehensive palliative care centers where pain relief is available, and a network of volunteer health aids who provide home health care. Recently this program has inspired some change in opioid regulation at the national level.
Another pharmaceutical trend in palliative care in many high income nations is that increasingly the dying are medicated for anxiety as well as pain, in order to make the experience less stressful for the family who are not accustomed to seeing the agitation that eminent death can bring among the dying.
Palliative care is also shaped by disclosure practices, which vary widely. In much of the world it is common practice for family to keep information about negative prognosis from the dying because this knowledge will dampen their health and spirit (Gordon and Paci 1997). Nondisclosure can seems problematically paternalistic and highly antithetical to notions of autonomy and consent so valued in many high-income nations. However, if we understood nondisclosure as part of the ecology of family care necessary in many low-income nations we can see how this this ethic serves to maintain the emotional well being of family groups. In some cases palliative care has in fact been structured around non-disclosure. For instance, in Thailand there are hospice care is provided without the explicit disclosure of imminent death to the patient (Stonington 2013).
6.3 Assisted dying
While, death is governed less than reproduction, euthanasia (pharmaceutical death administered by physicians) and assisted suicide (pharmaceutical death carried out by and within the family of the dying) provoke reaction, controversy and legal regulation, even though they affect only a tiny proportion of the terminally ill, and account for only a tiny fraction of all suicides. As mentioned above in the section on suicide, in the context of the imperatives of modern nation states to produce large populations as working and fighting forces, assisted dying becomes problematic in that it locates control over death between the dying and their families, leaving less control to medical, religious or state institutions (Foucault 2003). Nonetheless, pressure brought on policymakers over these issues can be a catalyst for the improvement of palliative care services—as in Australia, where the federal overturning of a Northern Territory euthanasia law in 1996 may have had the effect of increasing national funding for end-of-life care (ref).
There is some momentum globally to legalize and regulate both euthanasia, and assisted suicide under the umbrella term assisted dying, although in some locales where assisted dying has been legal, stricter controls are under consideration, e.g. Switzerland (Economist Report, Lein Foundation Page 18). At this time however there are only eight nations where forms of assisted dying are permitted (Columbia, Switzerland, Canada, Albania, The Netherlands, Belgium, Luxembourg) and in some cases liked he US, these are not federal but state level laws that permit these practices.
6.4 New Technologies of Death and Dying
One of the most noted changes in death in the last century has been movement of death to hospitals and clinics in the developed world and the addition of new technologies that bring new existential categories into being. These technologies and categories have reshaped how and when people die, providing new experiences of death. The mechanical ventilator for example has produced the category of brain death. The newness of these technologies comes with a sense of them as artificially assisting the prolongation of life and impeding “natural” death. This sense or being hooked to machines, is possibly the strongest in the developed world where the availability and ubiquity of these technologies it highest. In these contexts, dying with dignity often involves dying autonomous of machines (Roberts 2009). In less resourced contexts, there tend to be fewer concerns about the artificiality of these technologies, with more focus on how these technologies can strengthen family relationship through intensive care for the dying (Stonington 2013).
To provide contrastive examples, hospital death in the United States is often filled with fears of the inevitable dependence on machines, which is almost over determined through how hospital’s are organized within a nexus of ventilators, insurance reimbursement codes, state legislation, and pain relief (Kaufman 2005). This is not the case however, in Northern Thailand where relatives insist on keeping their dying relative hooked to machines to pay off their “debt of life” and at the last possible second bring them to die at home, where they can die surrounded by loved ones and their possessions. In these cases, machines like mechanical ventilators are not experienced as new problematic impositions but as a means to expend resources to pay off family debts (Stonington 2013) (similar to assisted reproduction discussed in section 3).
In a similar vein, in the United States the recent category of brain death produced through the mechanical ventilator was accepted rather easily which allowed for organ procurement and distribution. This acceptance came about within the context of concerns about skyrocketing hospital costs (Economist Lein foundation, 16). The category of brain death, allowed mechanical ventilators to be turned off after organ procurement, instead of maintain patients in vegetative states. In Japan, where death is experienced more through kin groups than through individuals, and where health care expenditure is rigorously controlled, a brain dead patient surrounded by a distraught family was not regarded as wasting scarce resources. Additionally, given the focus on family groups, the arrival of brain death was troubling giving that sharing organs with strangers had little appeal (Lock 2002).
The social science literature examining these technologies demonstrate that death and dying is not a stable state universally agreed on moment or condition… even in clinical medicine, which prides itself on universal and stable objects and categories, devoid of politics and history (Kaufman and Morgan 2005).
6.5 Conclusions
As with many of the “contours of human life” examined in this chapter, death and dying constitute an intimate and complex admixture of biomedical, social, and personal elements that are in the process of varying rates and directions of change and transformation. As in other domains, wealth and poverty are factors in determining not only when and from what cause death will occur but also the experience of dying, with a notable deficit in palliation for the under-resourced. Abundance of resources, however, may introduce drawbacks also, in the form of over-reliance on institutional care and life-extending efforts that go past the point of diminishing returns, spurring interest in alternatives emphasizing palliation and in some cases assisted dying. The advent of technologies that sustain life processes after permanent loss of consciousness, used to enhance successful organ transplantation, creates new existential categories whose contours remain contested.
Chapter Conclusion
The “contours of human life”, including childhood and adolescence, reproduction, the experience of disability and chronic conditions, and death – have been constant throughout human history. They will remain so, but scientific, social, and environmental changes are affecting their timing, texture, and patterns.
There is much to celebrate in these trends. Most populations are living longer. Child mortality has decreased enormously in recent decades, even in some of the poorest countries. Where overpopulation was only recently among humankind’s greatest concerns, birth rates have fallen. Science offers the prospect of welcome enhancements in coming decades. For many, more extensive use of palliation has eased the agony of dying.
These advances, however, are not universally shared. Serious inequalities persist in longevity, morbidity and disability, control over reproduction and sexuality, and in care at the end of life, and some of these disparities are widening, and the availability of enhancements could exacerbate these injustices. Vigilant monitoring of these inequalities, combined with forceful engagement with their economic and social determinants, will be needed to ensure that the favorable trends in the contours of human life become each person’s birthright.
References
Adam, D. 2013. “Mental Health: On the Spectrum.” Nature 496 (7446): 416–18. doi:10.1038/496416a.
Adetunji , J.and E. R.Bos. 2006. “Levels and Trends in Mortality in Sub-Saharan Africa: An Overview.” In Dean T Jamison, Richard G Feachem, Malegapuru W Makgoba, Eduard R Bos, Florence K Baingana, Karen J Hofman, and Khama O Rogo (eds.), Disease and Mortality in Sub-Saharan Africa. Washington D.C: World Bank.
Akyeampong, E., Hill, A. and Kleinman, A (Eds) (2015). Culture, Mental Illness and Psychiatric Practice in Africa. Indiana University Press
Allotey, P., Reidpath, D.D 2015. Sexual and Reproductive Health and Rights Post 2015--Challenges and Opportunities. BJOG: An International Journal of Obstetrics and Gynaecology 122(2): 152–155.
Allotey, P.A., Simone Diniz, Jocelyn Dejong, et al. 2011. Sexual and Reproductive Health and Rights in Public Health Education. Reproductive Health Matters 19(38): 56–68.
Allotey, P. and Gyapong, M. (2005). The gender agenda in the control of tropical diseases: A review of current evidence. Geneva: WHO/TDR.
Allotey P, Reidpath D, Kouamé A, Cummins R. 2003. The DALY, context and the determinants of the severity of disease: an exploratory comparison of paraplegia in Australia and Cameroon. Soc Sci Med 1982. 2003 Sep;57(5):949–58
Aryeetey, E and Kanbur, R. In Press. The Economy of Ghana: Sixty Years after Independence. Oxford: Oxford University Press.
Asad, T., 2007. On suicide bombing. New York: Columbia University Press
Asada, Y., Health Inequality: Morality and Measurement. 2007, Toronto: University of Toronto Press.
Asiaweek, 1993. Malaysia: Where Big Is Still Better. For Malays, Large Families Are Part of the Plan. 30
Association of Faculties of Medicine of Canada (2009), Primer on Population Health.
Balarajan, Y., U. Ramakrishnan, E. Özaltin, A. H. Shankar and S. V. Subramanian. 2011. “Anaemia in low-income and middle-income countries,” The Lancet 378: 2123-2135.
Barker D (1989). The rise and fall of western disease. Nature 338: 371-372
Barnett, K., et al (2012). Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. The Lancet, DOI:10.1016/S0140- 6736(12)60240-2
Ben-Shlomo Y, Davey Smith G. (1991): 'Deprivation in Infancy or in Adult Life: Which is more Important for Mortality Risk?, Lancet, 337: 530-4.
Barker D (1990). The fetal and infant origins of adult disease: the womb may be more important than the home. BMJ. 301(6761): 1111.
Barker D (1991). 'The Foetal and infant Origins of Inequalities in Health in Britain', Journal of Public Health Medicine, 13: 64-8.
Barker D (ed) (1992). The fetal and infant origins of adult disease. London: BMJ Publications.
Barker D (2013). The developmental origins of adult disease. Journal of the American College of Nutrition, 23:sup6, 588S-595S.
Bedford, Kate. 2009. Developing Partnerships: Gender, Sexuality and the Reformed World Bank. Minneapolis: University of Minnesota Press.
Berer, Marge, 2011. Repoliticising Sexual and Reproductive Health and Rights. Reproductive Health Matters 19(38): 4–10.
Bloom, D.E., D. Canning, and J. Sevilla, The effect of health on economic growth: A production function approach. World Development, 2004. 32(1): p. 1-13.
Bogardus C (l993) Insulin resistance in the pathogenesis of NIDDM in Pima Indians. Diabetes Care, 16(1):228-231.
Bostrom, Nick., Shulman, Carl. Embryo Selection for Cognitive Enhancement: Curiosity or Game-changer? Global Policy, Vol. 5, No. 1 (2014): 85-92
Braveman, P.A., Cubbin, C., Egerter, S., Williams, D.R. and Pamuk, E. 2010. Socioeconomic Disparities in Health in the United States: What the Patterns Tell Us. American Journal of Public Health, Vol. 100, No. S1, pp. S186-S196
Bukhman, G., Mocumbi, A.O., Horton, R. (2015). Reframing NCDs and injuries for the poorest billion: a Lancet Commission. Lancet, 386: 1221-1222.
Carey, N (2011). The epigenetics revolution: how modern biology is rewriting our understanding of genetics, disease and inheritance. London: Icon..
Case A, Deaton A (2015). Rising morbidity and mortality in midlife among white non-Hispanic Americans in the 21st century. PNAS 112: 15078-15083
Chi, B.H., Stringer, J. S. S. and D. Moodley. 2013. ”Antiretroviral Drug Regimens to Prevent Mother-to-Child Transmission of HIV: A Review of Scientific, Program, and Policy Advances for Sub-Saharan Africa.” Current HIV/AIDS Reports. June 2013, Volume 10, Issue 2, pp 124-133
Cohen G.A. (1989). On the Currency of Egalitarian Justice. Ethics, 99(4):906-44.
Commission on the Social Determinants of Health. (2008) Closing the gap in a generation. Health equity through action on the social determinants of health. Geneva: WHO 2008
Conklin, B. A. and L. M. Morgan. 1996. Babies, Bodies, and the Production of Personhood in North America and a Native Amazonian Society Ethos vol. 24 no 4: 657-94.
Daniels, N. “Normal Functioning and the Treatment-Enhancement Distinction” Cambridge Quarterly of Healthcare Ethics 9 (3):309--322 (2000)
Davey Smith G (2012). Epigenetics for epidemiologists: does evo-devo have implications for population health research and practice? International Journal of Epidemiology 41:236–247
de-Graft Aikins, A and Koram, K. In Press. Health and Healthcare in Ghana, 1957-2017. In E. Aryeetey and R.Kanbur (Eds). The Economy of Ghana: Sixty Years after Independence. Oxford: Oxford University Press
de-Graft Aikins, A and Agyemang, C. (Eds), 2016. Chronic non-communicable diseases in low and middle income countries. Oxon: CABI Publishers
de-Graft Aikins, A. 2015. Mental illness and destitution in Ghana: a social psychological perspective. In Emmanuel Akyeampong, Alan Hill and Arthur Kleinman. (Eds). The Culture of Mental Illness and Psychiatric Practice in Africa. Bloomington: Indiana University Press. (pages 112-143)
De Kok, B, Jeffery P. And Hussein, J. (Eds) 2010. Part Special Issue: Joining-up thinking: Loss in childbearing from interdisciplinary perspectives. Social Science & Medicine, 71, 10, Pages 1703- 1896
de Onis, M., M. Blössner and E. Borghi. 2010. “Global prevalence and trends of overweight and obesity among preschool children,” The American Journal of Clinical Nutrition 92: 1257-1264.
Durkheim, E., 1897. Le suicide; étude de sociologie. Paris,: F. Alcan.
Erikson, S. L. 2012. Global Health Business: The Production and Performativity of Statistics in Sierra Leone and Germany. Medical Anthropology, 32(4):367-384.
European Union. 2013. Health inequalities in the EU — Final report of a
consortium. Consortium lead: Sir Michael Marmot. European Commission Directorate-General for Health and Consumers.
Faber, N.S., Savulescu, J. And Douglas, T. 2016. “Why is Cognitive Enhancement Deemed Unacceptable? The Role of Fairness, Deservingness, and Hollow Achievements.” Frontiers in Psychology, 7:232. doi: 10.3389/fpsyg.2016.00232
Farmer, P. Infections and Inequalities: The Modern Plague. Berkeley, CA: University of California Press.
Faydi, E., Funk, M., Kleintjes, S., Ofori-Atta, A., Ssbunnya, J., Mwanza, J.,… Flisher, A. (2011). An assessment of mental health policy in Ghana, South Africa, Uganda and Zambia. Health Research Policy and Systems, 9(17), 2-11.
Fleishman, S. 2012. “Insomnia: Medicalization of Sleep May Be Needed.” Nature 491 (7425): 527–527. doi:10.1038/491527d.
Flores, G., Lin, H. 2013. Trends in racial/ethnic disparities in medical and oral health, access to care, and use of services in US children: has anything changed over the years? International Journal for Equity in Health, 12:10
Foucault, M. 1990. The History of Sexuality. New York: Vintage Books.
Foucault, M. 2003. Society Must be Defended: Lectures at the College de France, 1975-76. New York: Picador.
Fraser, Lin, Dan H. Karasic, Walter J. Meyer, and Kevan Wylie. 2010. “Recommendations for Revision of the DSM Diagnosis of Gender Identity Disorder in Adults.” International Journal of Transgenderism 12 (2): 80–85. doi:10.1080/15532739.2010.509202.
Fries J (1980) Aging, Natural Death, and the Compression of Morbidity. New England Journal of Medicine, 303(3), 130-135.
Geissler, P. W. 2013. “The Archipelago of public health. Comments on the landscape of medical research in 21st century Africa., In Ruth Jane Prince & Rebecca Marsland (ed.), Making and Unmaking Public Health in Africa: Ethnographic and Historical Perspectives. Ohio University Press. 231 – 256
Georges, E., 1996. Fetal ultrasound imaging and the production of authoritative knowledge in Greece. Medical Anthropology Quarterly 10(2):157-175.
Geyer S, Hemström O, Peter R, Vågerö D (2006). Education, income, and occupational class cannot be used interchangeably in social epidemiology. Empirical evidence against a common practice. Journal of Epidemiology and Community Health 60:804-10.
Goesling B, Firebaugh G (2004). The trends in inequality in health. Population and development review, 30:131–146
Gordon, D., 1988. Tenacious assumptions in western medicine. In Biomedicine Examined: Culture, Illness, and Healing. M. M. Lock and D. R. Gordon, eds. Pp. 19-56. Dordrecht ; Boston: Kluwer Academic Publishers.
Gordon, D.R., and Eugenio Paci, 1997. Disclosure practices and cultural narratives: understanding concealment and silence around cancer in Tuscany, Italy. Social Science and Medicine 44(10):1443-1452.
Greenberg, G. 2010. Manufacturing Depression: The Secret History of an American Disease. New York: Simon & Schuster.
Greenhalgh, S., Just one child : science and policy in Deng's China. 2008, Berkeley:
University of California Press. xxii, 403 p., 6 p. of plates.
Grundy, T., 2014. Kissing corpses is helping spread Ebola, expert says. In Religion Service News. London.
Gwatkin DR et al. (2007). Socio-economic differences in health, nutrition, and population within developing countries: an overview. Washington, DC, The World Bank.
Hall, R.E. (Ed), 2013. The melanin millennium: Skin color as 21st century international discourse. New York, NY, US: Springer Science + Business Media, 348 pp
Hall, V., Thomsen, R.W., Henriksen, O. And Lohse, N. (2011). Diabetes in Sub Saharan Africa 1999-2011: epidemiology and public health implications: a systematic review. BMC Public Health, 11:564.
Hamdy, S., 2016. All Eyes on Egypt: Islam and the Medical Use of Dead Bodies Amidst Cairo’s Political Unrest. Medical Anthopology 35(3):220-235.
Henshaw H., Sharkey L, Crowe D, Ferguson M. Research priorities for mild-to-moderate hearing loss in adults. The Lancet. 2015 Nov;386(10009):2140–1.
Global Burden of Disease Pediatrics, C. 2016. “Global and national burden of diseases and injuries among children and adolescents between 1990 and 2013: Findings from the global burden of disease 2013 study,” JAMA Pediatrics 170: 267-287.
Heckman J. Stixrud J, Urzua S (2006) The Effects of Cognitive and Noncognitive Abilities on Labor Market Outcomes and Social Behavior. Journal of Labor Economics vol 24, no. 3
Hoile, Oksana V., Gill Green, Sushil Jathanna, and Tom Stewart 2002. Violence against Women. The Lancet 360(9329): 343.
Hosseinpoor AR, Mohammad K, Majdzadeh R, Naghavi, Abolhassani F, Sousa A, Speybroeck N, Jamshidi HR, Vega J. (2005) Socioeconomic inequality in infant mortality in Iran and across its provinces. Bulletin of the World Health Organization 2005; 83:837-844.
Houweling, Tanja A.J.(2007). Socio-economic inequalities in childhood mortality in low and middle income countries. Doctoral thesis, Erasmus University Medical Center, Rotterdam, The Netherlands
Houwelling T.A.J., A. E. Kunst, and J. P. Mackenbach (2003), Measuring Health Inequality among Children in Developing Countries: Does the Choice of the Indicator of Economic Status Matter?, International Journal for Equity in Health 2(8).
Idele, P., A. Gillespie, T. Porth, C. Suzuki, M. Mahy, S. Kasedde and C. Luo. 2014. “Epidemiology of HIV and AIDS among adolescents: current status, inequities, and data gaps,” J Acquir Immune Defic Syndr 1: S144-53.
Ilieva, I.P, Cayce J. Hook, and Martha J. Farah “Prescription Stimulants' Effects on Healthy Inhibitory Control, Working Memory, and Episodic Memory: A Meta-analysis” Journal of Cognitive Neuroscience June 2015, Vol. 27, No. 6, Pages 1069-1089
IDF. The Global Diabetes Plan, 2011 – 2021. Brussels: IDF.
Juengst, Eric and Moseley, Daniel, "Human Enhancement", The Stanford Encyclopedia of Philosophy (Spring 2016 Edition), Edward N. Zalta (ed.).
Kadosh, Roi Cohen et al. The neuroethics of non-invasive brain stimulation Current Biology, Volume 22, Issue 4, R108 - R111
Kaufman, S., 2005. And a Time to Die : How American Hospitals Shape the End of Life. New York: Scribner.
Kaufman, Sharon, and Lynn Morgan, 2005. The Anthropology of the Beginnings and Ends of Life. Annual Review of Anthropology 34:317-341.
Kermack, AG McKendrick, and PL McKinlay (1934). Death-rates in Great Britain and Sweden. Some general regularities and their significance. The Lancet, 1934; 31 March: 698–703. Reprinted in International Journal of Epidemiology 2001; 30 :678–683
Kieling, C., H. Baker-Henningham, M. Belfer, G. Conti, I. Ertem, O. Omigbodun, L. A. Rohde, S. Srinath, N. Ulkuer and A. Rahman. 2011. “Child and adolescent mental health worldwide: evidence for action,” The Lancet 378: 1515-1525.
Kim, J-Y., J. V. Millen, A. Irwen and J. Gershman. 2001. Dying for Growth: Global Inequality and the Health of the Poor. Monroe, ME: Common Courage Press.
Klinenberg, Eric, 2002. Heat wave : a social autopsy of disaster in Chicago. Chicago: University of Chicago Press.
Krause, M. 2014. The Good Project. Humanitarian NGOs and the Fragmentation of Reason. Chicago: Chicago University Press
Kuh D, Ben Shlomo Y (2004). A life course approach to chronic disease epidemiology. Second edition. Oxford: Oxford University Press.
The Lancet. Hearing loss: an important global health concern. The Lancet. 2016 Jun;387(10036):2351
Lang, Tim, and Michael Heasman, 2016. Food wars : the global battle for mouths, minds and markets. London ; New York: Routledge.
Langford, Jean, 2016. Medical Eschatologies: The Christian Spirit of Hospital Protocol. Medical Anthopology 35(3):236-246.
Laplante D, Barr RG, Brunet A, Galbaud Du Fort G, Meaney ML, Saucier J-F, Zelazo P, King S. (2004) “Stress During Pregnancy Affects General Intellectual and Language Functioning in Human Toddlers.” Pediatric Research 56: 400–410
Larsson, J. 2007. Prioriteringar i hälso- och sjukvården. Socialstyrelsen analys och slutsatser utifrån rapporten ”Vårdens alltför svåra val?”. 2007-103-4. Socialstyrelsen.
Laudan, Rachel, 2015. A Plea for Culinary Modernism. . In Jacobin.
Layne, Linda L. 2003. Motherhood Lost: A Feminist Account of Pregnancy Loss in America. New York: Routledge.
Le Clair, J, 2012. Introducing global organizational change in sport and the shifting meaning of disability. In J. Le Clair (Ed), Disability in the Global Sport Arena. A Sporting Chance. Oxon: Routledge.
Le Grand, J., 1987. Inequalities in health. European Economic Review, 31: p. 182-91.
Leinsalu M, Vågerö D, Kunst A (2003). Estonia 1989-2000: enormous increase in mortality differences by education. Int J Epidemiol. 2003 32:1081-7.
Leinsalu M, Stirbu I, Vågerö D, Kalediene R, Kovacs K, Wojtyniak B, Wroblewska V, Makenback J, Kunst A (2009). Educational inequalities in mortality in four Eastern European countries: divergence in trends during the post-communist transition from 1990 to 2000 International Journal of Epidemiology 2009; 38: 512–525
Leinsaul M, Vågerö D, Kunst A (2004). Increasing ethnic differences in mortality in Estonia after the collapse of the Soviet Union. Journal of Epidemiology and Community Health 58:583–589 .
Leone, T., Coast, E., Narayanan, S and de-Graft Aikins, A. (2012) Diabetes and depression comorbidity within poor settings in low and middle income countries (LMICs): a mapping of the evidence. Globalization and Health, 8:39.
Lichtenstein, Paul, Linda Halldner, Johan Zetterqvist, Arvid Sjölander, Eva Serlachius, Seena Fazel, Niklas Långström, and Henrik Larsson. 2012. “Medication for Attention Deficit–Hyperactivity Disorder and Criminality.” New England Journal of Medicine 367 (21): 2006–14. doi:10.1056/NEJMoa1203241.
Lippert-Rasmussen K, Eyal N. Equality and Egalitarianism. In: Ruth Chadwick, ed. Encyclopedia of Applied Ethics. 2nd ed. San Diego: Elsevier Academic Press, 2012:14148.
Livingston, Julie, 2012. Improvising Medicine: An African Oncology Ward in an Emerging Cancer Epidemic. Durham: Duke University Press.
Lock, Margaret M. 2002. Twice dead : organ transplants and the reinvention of death. Berkeley: University of California Press.
Lock, Margaret M., and Deborah Gordon, 1988. Biomedicine examined. Dordrecht ; Boston: Kluwer Academic Publishers.
Lumey LH, M. Khalangot, A. Vaiserman. 2015 . “Association between type 2 diabetes and prenatal exposure to the Ukraine famine of 1932–33: a retrospective cohort study.” The Lancet Diabetes and Endocrinology Volume 3, No. 10, p787–794
Macer, D. 2012. Ethical consequences of the positive views of enhancement in Asia. Health Care Analysis, 20(4): 385-397. doi:http://dx.doi.org/10.1007/s10728-012-0230-3
Marchard, S., D. Wiker and B. Landesman. 1998. “Class, health and justice,” The Milbank Quarterly 76: 449-467.
Mackenbach JP, Bos V, Andersen O, Cardano M, Costa G, Harding S, Reid A, Hemström Ö, Valkonen T, Kunst AE: Widening socioeconomic inequalities in mortality in six Western European countries. Int J Epidemiol 2003, 32(5):830–837.
Mackenbach J, Stirbu I, Roskam AR, Schaap M et al (2008). Socioeconomic Inequalities in Health in 22 European Countries. N Engl J Med 2008;358:2468-81
Mark, M., 2014. As Ebola Epidemic tightens grip, West Africa turns to Religion for Succour. In The Guardian. U.K. .
Marmot, M. (2015). The Health Gap. London: Bloomsbury
McCoy, D., and Linsey McGoey. 2011. “Global Health and the Gates Foundation,” in O. D. Williams and S. Rushton (eds.), Partnerships and Foundations in Global Health Governance, London: Palgrave.
McCoy, D., S. Chand, and D. Sridhar. 2009. “Global Health Funding: How Much, Where It Comes from and Where It Goes.” Health Policy and Planning 24 (6): 407–17.
McGoey, L, Reiss, J. and Wahlberg, A. 2011. The Global Health Complex. BioSocieties 6(1): 1-9.
Mokdad, A.H. et al. 2016. Global burden of diseases, injuries, and risk factors for young people's health during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet, 387 (10036): 2383–2401.
Mofenson, L. M. and M. F. Cotton. 2013. “The challenges of success: adolescents with perinatal HIV infection.” Journal of the International AIDS Society 16: 1-3.
Morgan, Lynn, 1989. When Does Life begin? A Cross-Cultural Perspective on the Personhood of Fetuses and Young Children. In Abortion Rights and Fetal Personhood. E. Doerr and J. W. Prescott, eds. Pp. 89-107. Long Beach, California: Centerline Press.
Moser K, Shkolnikov V, Leon D (2005). World mortality 1950-2000: divergence replaces convergence from the late 1980s. Bull World Health Organ. 2005 Mar;83(3):202-9
Moynihan, Ray, Iona Heath, and David Henry. 2002. “Selling Sickness: The Pharmaceutical Industry and Disease Mongering.” BMJ : British Medical Journal 324 (7342): 886–91.
Murphy M, Bobak M, Nicholson A, Rose R, Marmot M (2006). The widening gap in mortality by educational level in the Russian Federation, 1980-2001. Am J Public Health. 2006 96: 1293-1299.
Murray, C. J., R. M. Barber, et al (2015). "Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990-2013: quantifying the epidemiological transition." Lancet 386(10009): 2145-2191.
Muthumbi, J. et al. 2015. Female Genital Mutilation: A Literature Review of the Current Status of Legislation and Policies in 27 African Countries and Yemen. African Journal of Reproductive Health September 2015; 19 (3): 32-40
Norheim, O.F., Gini impact analysis: measuring pure health inequity before and after interventions. Public Health Ethics, 2010. 3(3): p. 282-92.
Norheim, O. F., P. Jha, K. Admasu, T. Godal, R. Hum, M. Kruk, O. Gómez-Dantés, C. Mathers, H. Pan, J. Sepúlveda, W. Suraweera, S. Verguet, A. Woldemariam, G. Yamey, D. Jamison and R. Peto (2015). "Avoiding 40% of the premature deaths in each country, 2010–30: review of national mortality trends to help quantify the UN Sustainable Development Goal for Health." Lancet 385(January 17): 239-252.
Nyarko, Y, Goldfrank, L., Ogedegbe, G., Soghoain, S., de-Graft Aikins, A. and NYU-UG-KBTH Ghana Ebola Working Group. 2015. Preparing for Ebola Virus Disease in West African Countries not yet affected: Perspectives from Ghanaian Health Professionals. Globalization and Health,11:7, doi: 10.1186/s12992-015-0094-z
Olumide, YM; Akinkugbe, AO; Altraide, D; Mohammed, T; Ahamefule, N; Ayanlowo, S; Onyekonwu, C; Essen, N (April 2008). "Complications of chronic use of skin lightening cosmetics". International Journal of Dermatology 47 (4): 344–53.doi:10.1111/j.1365-4632.2008.02719.x.PMID 18377596.
Office of Population Censuses and Surveys (1995). Occupational health. The Registrar Generals decennial supplement for England and Wales. Edited by Frances Drever. London: HMSO 1995
Olshansky SJ, Antonucci T, Berkman L, Binstock R et al. Differences in life expectancy due to race and education are widening and many may not catch up. Health affairs 2012
Paton, G.C. et al. 2016. Our future: a Lancet commission on adolescent health and wellbeing. Lancet, 387 (10036): 2423–2478
Pembrey M, Saffery R, Bygren LO, Network in Epigenetic Epidemiology (2014). Human transgenerational response to early-life experience: potential impact on development, health and biomedical research. J Med Gen 51:563-572.
Peto, R., A.D. Lopes, and O.F. Norheim, Halving premature death. Science, 2014. 345(6202): p. 1272.
Pfeiffer, J. and Chapmann, R. 2010. “Anthropological Perspectives on Structural Adjustment and Public Health”, Annual Review of Anthropology, Vol. 39: 149-165
Poku, N. 2006. AIDS in Africa: How the Poor are Dying. Cambridge, UK: Polity Press.
PolicyCures. 2015. “Neglected Disease Research and Development: The Ebola Effect”. Available via: http://policycures.org/gfinder.html
Powell, R.A., Mwangi-Powell, F.N., Radbruch, L. et al 2015. “Putting palliative care on the global health agenda.” Lancet Oncology, 16(2) 131-133
Preston, S., P. Heuveline, and M. Guillot, Demography: Measuring and Modeling Population Processes. 2001, Oxford: Blackwell Publishers.
Prince, M., Patel, V., Saxena, S., Maj, M., Maselko, J., Phillips, M. R., & Rahman, A.(2007). No health without mental health. Lancet, 370, 859-77.
Reidpath DD, Allotey PA, Kouame A, Cummins RA. 2003. Measuring health in a vacuum: examining the disability weight of the DALY. Health Policy Plan.18(4):351–6
Rees, T. 2014. “Humanity/Plan; or, On the "Stateless" Today (Also Being an Anthropology of Global Health)” Cultural Anthropology 29, 3: 457-478
Roberts, F.S. Elizabeth , 2009. American Death. Focaal—European Journal of Anthropology 54:114-119.
Robinson, Julia, and James Pfeiffer, 2015. The IMF’s Role in the Ebola Outbreak – The Long-Term Consequences of Structural Adjustment. In Global Research.
Roisman, G. I and R. C. Fraley, 2012. The legacy of early interpersonal experience. Adv Child Dev Behav 2012;42:79-112.
Saxena, S., Lora, A., Morris, J., Berrino, A., Esparza, P., Barrett, T., van, O.M., & Saraceno, B. (2011). Mental health services in 42 low- and middle-income countries: a WHO-AIMS cross-national analysis. Psychiatr.Serv., 62(2), 123-125.
Scheffler, Richard M, Timothy T Brown, Brent D Fulton, Stephen P Hinshaw, Peter Levine, and Susan Stone. 2009. “Positive Association between Attention-Deficit/ Hyperactivity Disorder Medication Use and Academic Achievement during Elementary School.” Pediatrics 123 (5): 1273–79. doi:10.1542/peds.2008-1597.
Schelle, K.J., Faulmüller, N., Caviola, L and Hewstone, M. 2014. Attitudes toward pharmacological cognitive enhancement—a review. Frontiers in Systems Neuroscience, 8:53. doi: 10.3389/fnsys.2014.00053
Scheper-Hughes, Nancy. 1993. Death without Weeping: The Violence of Everyday Life in Brazil. Berkeley, CA: University of California Press.
Scheper-Hughes, Nancy, 1992. Death Without Weeping: The Violence of Everyday Life in Brazil. Berkeley: University of California Press.
Sen, A.K. and J.E. Foster, On economic inequality. Expanded edition with a substantial annexe by James E. Foster. 1997, Oxford.: Clarendon Press.
Singer, Merrill, and Hans Baer, 1995. Critical medical anthropology. Amityville, N.Y.: Baywood Pub. Co.
Shkolnikov V, Andreev E, Jdanov D, Jasilionis D, Kravdal Ö, Vågerö D, Valkonen T. Increasing absolute mortality disparities by education in Finland, Norway and Sweden, 1971-2000. Journal of Epidemiology and Community Health 2012
Smith, S.S et al (2012). Managing patients with multimorbidity: systematic review of interventions in primary care and community settings. BMJ, 345:e5205 doi: 10.1136/bmj.e5205
Smits, J. and C. Monden, Length of life inequality around the globe. Soc Sci Med, 2009. 68: p. 1114-23.
Staples, J., and T. Widger, 2012. Situating suicide as an anthropological problem: ethnographic approaches to understanding self-harm and self-inflicted death. Culture Medicine and Psychiatry 36(2):183-203.
Steingraber, S. 2007. The falling age of puberty in US girls: What we know, what we need to know. Breast Cancer Fund.
Steingrímsdóttir ÓA, Næss Ø, Moe JO, Grøholt E-K, Thelle DS, Strand BH, Bævre K: Trends in life expectancy by education in Norway 1961–2009. Eur J Epidemiol 2012, 27(3):163–171.
Stevenson, L., 2014. Life beside itself : imagining care in the Canadian Arctic. Oakland, California: University of California Press.
Stonington, S., 2013 “The debt of life: Thai lessons on a process-oriented ethical logic.". New England Journal of Medicine 369(17):1583-1585.
Stonington, S. 2015 On the (f)utility of pain. The Lancet 385(1388-1389)
Susser M, Levin B. 1999. Ordeals for the fetal programming hypothesis: The hypothesis largely survives one ordeal but not another. Editorial. British Medical Journal 318(7188): 885–886.
Tarlo, E., Unsettling memories : narratives of the emergency in Delhi. 2003, Berkeley: University of California Press. x, 234 p., [28] p. of plates.
Taylor, J.S., Layne, L.L. and Wozniak, D.F. 2004. Consuming motherhood. New Brunswick, N.J.: Rutgers University Press.
Timonin S, Shkolnikov V, Jasiolinis D, Grigoriev P, Jdanov D, Leon D (2016). Disparities in length of life across developed countries: measuring and decomposing changes over time within and between country groups. Population Health Metrics 14 (29):1-19.
Tomkins, A., Duff , J., Fitzgibbon, A., Karam, A., Mills, E.J., Munnings, K., Smith, S., Seshadri, S.R., Steinberg, S., Vitillo, R., Yugi, P. 2015. Controversies in faith and health care. Lancet, 386: 1776–85.
UNICEF. 2012. Progress for Children: A Report Card on Adolescents, New York: UNICEF.
UNICEF. 2013. Female Genital Mutilation, New York: UNICEF.
UNICEF. 2014. Committing to Child Survival: A Promise Renewed. New York: Unicef.
UNICEF. 2014. Inequality in Ghana: A Fundamental National Challenge
Briefing Paper - April 2014. Accessible via: http://www.undp.org/content/dam/ghana/docs/Doc/Inclgro/Ghana-unicef%20Inequality%20Briefing%20Paper%20FINAL%20DRAFT%20Apr%202014.pdf (last accessed: 06/07/2016)
UNICEF. 2015. Committing to Child Survival: A Promise Renewed. Progress Report 2015.
UNICEF. 2015. Children & AIDS: 2015 Statistical Update, Global Charts and Figures, available via: http://data.unicef.org/hiv-aids/emtct.html
United Nations, Department of Economic and Social Affairs, Population Division Adolescent Fertility Trends, December 2013 http://www.un.org/en/development/desa/population/publications/pdf/popfacts/PopFacts_2013-7_new.pdf
United Nations, Department of Economic and Social Affairs, Population Division, World Population Prospects The 2015 Revision, Volume I: Comprehensive Tables, 2015
United Nations, Department of Economic and Social Affairs, Population Division Adolescent Fertility since the International Conference on Population and Development (ICPD) in Cairo 2013
United Nations. 2012. World Population Monitoring: Adolescents and Youth, A Concise Report. New York: United Nations.
United Nations. The Millennium Development Goals Report 2015. New York 2015. http://www.un.org/millenniumgoals/2015_MDG_Report/pdf/MDG%202015%20rev%20%28July%201%29.pdf . Accessed on May 16th 2016.
United Nations. Sustainable Development Goals. https://sustainabledevelopment.un.org/sdgs. Accessed on May 16th 2016
United Nations Population Division, World Population Prospects: The 2012 Revision, 2012, United Nations: Washington.
Vågerö D, Illsley R. 1995. Explaining Health Inequalities: Beyond Black and Barker. European Sociological Review, Vol. 11: 219-241
Vågerö D, Erikson R (1997) Socioeconomic differences in morbidity and mortality in western Europe The Lancet 350(9076):516;
Vågerö D. 2008. Closing the global health gaps in a generation- how is it possible? Editorial. International Journal of Public Health 53:279-280
Vågerö D (2010). The east west health divide in Europe: growing and shifting eastwards. European Review, Vol. 18, No. 1, 23–34 r 2010
Vågerö, D., Koupil, I., Parfenova, N., Sparén, P. 2013. Long-term health consequences following the siege of Leningrad. In L. H. Lumey and Alexander Vaiserman (Eds), Early Life Nutrition and Adult Health and Development: Lessons from Changing Dietary Patterns, Famines and Experimental Studies. New York, Nova Science Publishers. 207-225.
Velleman, J. D. 1991. "Well-being and time." Pacific Philosophical Quarterly 72(1): 48-77
Victora CG, Wagstaff A, Schellenberg JA, Gwatkin D, Claeson M, Habicht JP (2003). Applying an equity lens to child health and mortality: more of the same is not enough. Lancet , 362: 233–241
Vilarim MM, Rocha Araujo DM, Nardi AE (2011). "Caffeine challenge test and panic disorder: A systematic literature review". Expert Review of Neurotherapeutics 11 (8): 1185–95. doi:10.1586/ern.11.83. PMID 21797659.
Wagstaff A. Socio-economic inequalities in child mortality: comparison across nine developing countries. Bull World Health Organ, 2000, 78: 19-29.
Wakefield, J C. 1992. “The Concept of Mental Disorder. On the Boundary between Biological Facts and Social Values.” The American Psychologist 47 (3): 373–88.
Wan Ibrahim WA, Zainab I, Redzuan M. Living arrangement of older population in rural Malaysia. Adv Nat Appl Sci. 2012;6(3 SPECL.ISSUE 2):383–7
Wang, H., C. A. Liddell, M. M. Coates, et al. 2016. “Global, regional, and national levels of neonatal, infant, and under-5 mortality during 1990 and 2013: a systematic analysis for the Global Burden of Disease Study 2013,” The Lancet 384: 957-979.
Wang, Y. and T. I. M. Lobstein. 2006. “Worldwide trends in childhood overweight and obesity,” International Journal of Pediatric Obesity 1: 11-25.
Warin, M., V. Moore, T. Zivkovic and M. Davies. 2011. Telescoping the origins of obesity to women's bodies: How gender inequalities are being squeezed out of Barker's hypothesis. Annals of Human Biology 38: 453-460.
Wasserman, D., Q. I. Cheng and G.-X. Jiang. 2005. “Global suicide rates among young people aged 15-19,” World Psychiatry, 4: 114-120.
Wasson K. 2011. “Medical and genetic enhancements: ethical issues that will not go away.” Am J Bioeth. 11(1):21-2. doi: 10.1080/15265161.2011.566671
Watson, K., Safe and sustainable roads: The case for a sustainable development goal, 2012. London: FIA Foundation.
Weeks, J.R., Hill, A.G., Stoler, J. (Eds.). 2013. Spatial Inequalities: Health, Poverty, and Place in Accra, Ghana. Dordrecht: Springer
Williams, O. D. and S. Rushton. 2011. “Private Actors in Global Health Governance,” in O. D. Williams and S. Rushton (eds.), Partnerships and Foundations in Global Health Governance, London: Palgrave.
Whyte, SR, MA Whyte, Lotte Meinert, and Jenipher Twebaze. 2013. “Therapeutic Clientship: Belonging in Uganda’s Mosaic of AIDS Projects.” In When People Come First: Critical Studies in Global Health. Princeton: Princeton University Press. pp. 140-165
WHO, Adolescents: Health Risks and Solutions, Factsheet, May 2014, Geneva: WHO. http://www.who.int/mediacentre/factsheets/fs345/en/
WHO. 2014. Health for the World’s Adolescents: A Second Chance in the Second Decade (Full Report), Geneva: WHO. http://apps.who.int/adolescent/second-decade/
WHO (2011). World Report on Disability. Geneva: WHO
WHO, 2011. Mercury in skin lightening products. Geneva: WHO (available at http://www.who.int/ipcs/assessment/public_health/mercury_flyer.pdf)
WHO Health for the World’s Adolescents: A Second Chance in the Second Decade (Executive Summary), Geneva: WHO. http://apps.who.int/adolescent/second-decade/files/1612_MNCAH_HWA_Executive_Summary.pdf
WHO Country Data on HIV and AIDS, 2008, Geneva: WHO. http://apps.who.int/globalatlas/predefinedReports/
WHO media release, Adolescents falling through gaps in HIV Services, 25 November 2013, Geneva: WHO. http://www.who.int/mediacentre/news/releases/2013/hiv-adolescents-20131125/en/
The World Wealth and Income Database, http://www.wid.world/
Xu M-Q, Sun W-S, Liu B-X, Feng G-Y, Yu L, Yang L, He G, Sham P, Susser E, St Clair D, He L (2009). Prenatal Malnutrition and Adult Schizophrenia: Further Evidence From the 1959-1961 Chinese Famine. Schizophr Bull 35(3): 568–576.
You, D. and D. Anthony. Generation 2025 and Beyond: The Critical Importance of Understanding Demographic Trends for Children of the 21st Century. Unicef Occasional Papers. No1, November (Unicef: 2012)
[1] Affiliations: University of Ghana, Ghana; Harvard University, USA.
[2] Affiliations: Monash University, Malaysia; University of Bayreuth, Germany; University of Sydney, Australia; Harvard University, USA; University of Wisconsin, USA; IIASA, Austria; University of Bergen, Norway; University of Michigan, USA; Stockholm University, Sweden.
[3] Affiliations: Institute for Futures Studies, Sweden.
[4] These cover each five-year time period from 1950 to 2015, where the last five-year period is partly estimated. There are separate life tables for each country, World Bank income regions, and the world as a whole. Since age distributions differ between countries, and within countries over time, all life tables are age-adjusted. For every fifth year from 1970 to 2010, we estimated the death rates in it by averaging the age-specific risks in the five-year periods before and after it (so our 1970 rates describe 1965-75); this smooths out any sudden mortality changes. It should be noted that many countries lack vital registration, so UNPD mortality trend estimates are only approximate.
[5] This terminology is important: Longevity is the expected actual age at death for each individual in a life table (and inequality in longevity can therefore be seen as an ex post measure), while life expectancy is an ex ante measure of average health for the whole population.
[6] We use the formula:
,
where yi is the age at death for the ith person, n is the number of people in the population (100 000 in our life table model), and m is average health (life expectancy at birth) in the population. We extracted the expected final distribution of people dying in different age groups from the ndx column in the life table.
[7] Life tables by sex are available from UNPD.
[8] The standard Ginih is population size invariant, and we have not adjusted for population size in the other results given below.
[9] See for example Michael Marmot: ”Health is improving globally. (...) Within many countries (…) inequalities in health are increasing – the health of the best off is increasing more rapidly than that of the worst off. The best and worst of times coexist.” Marmot M. The Health Gap. London: Bloomsbury 2015.
[10] It is important to note that the choice of health measure may affect our results. Both types of measures are important, and analysts should always make clear what kind of health inequalities are reported.
[11] For example, epilepsy, a neurological condition, is typically treated as a mental health disorder. Adults and children from poor and rural communities are more likely to get hospitalized in psychiatric institutions and alternative healing centres such as traditional shrines and prayer camps.
[12] Similar things are happening in Singapore, Japan, Italy – although most tend to give some one time small incentive rather than make affordable child care more widely available so women can work.
[13] http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2709326/. http://www.who.int/reproductivehealth/topics/unsafe_abortion/article_unsafe_abortion.pdf
[14] https://www.guttmacher.org/about/journals/ipsrh/2012/09/use-medicines-changing-face-abortion, Abortion facts. - http://www.guttmacher.org/pubs/fb_IAW.html
[15] Note on birth (birth attendance and c-section): Stratified reproduction shapes patterns of access to maternal health services and the quality of care received. Julio Frenk, former Minister of Health in Mexico, remarked in opening statements at the 2007 Women Deliver conference in London that maternal and child health are the best entry points to improvement of the health-care system, and crucial to maternal and child health is the quality of birth attendance. The issue of birth attendance has however frequently been contested. With the exception of sub-Saharan Africa, rates of births assisted by a medically trained attendant have shown impressive increases over the past 15–20 years and today data indicate that 59% of developing world births are assisted by a medically trained professional.7 The large majority of these births occur in a health facility.
Cesarean section is a surgical procedure intended for use when the life of the infant, or the mother is at risk. In 1985 the World Health Organization (WHO) stated: "There is no justification for any region to have CS rates higher than 10-15%".
[16] Air Force Special Operations Command Instruction 48–101 (sects. 1.7.4), U.S. Air Force Special Operations Command, November 30, 2012.
[17] “It is more plausible to view genetic engineering as the ultimate expression of our resolve to see ourselves astride the world, the masters of our nature. But that promise of mastery is flawed. It threatens to banish our appreciation of life as a gift, and to leave us with nothing to affirm or behold outside our own will.”
[18] Riktlinjerna exemplifierades med fyra prioriteringsgrupper: […] ”Prioriteringsgrupp IV Vård av andra skäl än sjukdom och skada”, p.9 (Larsson 2007)
The commenting phase has been concluded. We thank you for your thoughtful comments and responses.